ЛЕКЦИЯ N 12
ТЕМА: ПРАВОВАЯ И ДЕОНТОЛОГИЧЕСКАЯ ОЦЕНКА
ВРАЧЕБНЫХ
ОШИБОК И НЕСЧАСТНЫХ СЛУЧАЕВ В МЕДИЦИНЕ.
ЮРИДИЧЕСКОЕ И НАУЧНО-ПРАКТИЧЕСКОЕ
ЗНАЧЕНИЕ
МЕДИЦИНСКОЙ ДОКУМЕНТАЦИИ.
В очень сложной и ответственной
профессиональной врачебной деятельности,
могут встречаться случаи неблагоприятных
исходов медицинского вмешательства.
Чаще всего они обусловливаются тяжестью
самого заболевания или травмы,
индивидуальными особенностями организма,
поздней, не зависящей от врача, диагностикой
и , отсюда, запоздалым началом лечения.
Но иногда неблагоприятные исходы
медицинского вмешательства оказываются
следствием неправильной оценки
клинической симптоматики или неправильных
лечебных действий. В этих случаях
речь идет о ВРАЧЕБНЫХ ОШИБКАХ.
Большая медицинская энциклопедия
определяет врачебную ошибку , как
ошибку врача при исполнении своих
профессиональных обязанностей,
являющуюся следствием добросовестного
заблуждения и не содержащую состава
преступления или признаков проступков.
/Давыдовский И.В. с соавт.»Врачебные
ошибки» БМЭ-М 1976. т.4. С 442-444 /.
Следовательно, основным содержанием
понятия «врачебная ошибка»,
является ДОБРОСОВЕСТНОЕ ЗАБЛУЖДЕНИЕ
ВРАЧА в своих суждениях и действиях.
Это означает, что в конкретном случае
врач убежден, что он прав. При этом он
делает так, как требуется, делает
добросовестно. И все-таки ошибается.
Почему? Различают объективные и
субъективные причины врачебных ошибок.
Объективные причины не зависят от
уровня подготовки и квалификации врача.
При их наличии врачебная ошибка может
возникнуть и тогда, когда врач использует
все имеющиеся возможности для ее
предупреждения. К ОБЪЕКТИВНЫМ причинам
появления
врачебных ошибок относят: — недостаточное
развитие самой медицины, как науки /
имеется ввиду недостаточная изученность
этиологии, патогенеза, клинического
течения ряда заболеваний /,
— объективные трудности диагностики
/ необычное течение заболевания или
патологического процесса, наличие у
одного больного нескольких конкурирующих
заболеваний, тяжелое бессознательное
состояние больного и отсутствие времени
на обследование, отсутствие требующейся
диагностической аппаратуры /.
К СУБЪЕКТИВНЫМ причинам врачебных
ошибок, зависящих от личности врача и
степени его профессиональной подготовки,
относятся:- недостаточный практический
опыт и связанные с этим недооценка или
переоценка анамнестических данных,
результатов клинического наблюдения,
лабораторных и инструментальных методов
исследования, а так же переоценка врачом
своих знаний и возможностей.
Практика показывает, что опытные
врачи ошибаются только в очень сложных
случаях, а молодые врачи ошибаются и
тогда, когда случай следует считать
типичным.
ВРАЧЕБНАЯ ОШИБКА — категория не
юридическая. В действиях врача, приведших
к врачебной ошибке, не содержится
признаков преступления или проступка,
т.е. общественно опасных деяний в форме
действия или бездействия, причинивших
существенный /для преступления/ или
несущественный /для проступка/ вред,
охраняемым законом правам и интересам
личности, в частности — здоровью и
жизни. Поэтому за ошибку врач не может
быть привлечен ни к уголовной, ни к
дисциплинарной ответственности. В
полной мере это относится лишь к врачебным
ошибкам, имеющим в своей основе
ОБЪЕКТИВНЫЕ причины. Если же причины
являются СУБЪЕКТИВНЫМИ, т.е. связанные
с личностными или профессиональными
качествами врача, то прежде чем его
неправильные действия признать
ВРАЧЕБНОЙ ОШИБКОЙ, необходимо исключить
элементы небрежности и халатности, или
таких недостаточных знаний, которые
могут считаться медицинским невежеством.
Нельзя называть врачебной ошибкой
дефекты медицинской деятельности,
вызванные недобросовестными действиями
врача или неисполнением им своих
возможностей и возможностей лечебного
учреждения.
Все врачебные ошибки можно разделить
на следующие группы:
— диагностические ошибки,
— ошибки в выборе метода и проведения
лечения,
— ошибки в организации медицинской
помощи,
— ошибки в ведении медицинской
документации.
Некоторые авторы / Н.И. Краковский и
Ю.Я. Грицман » Хирургические ошибки
» М. Медицина, 1976 -С 19 /, предлагают
выделить еще один вид врачебных ошибок,
которые они назвали, ошибками в
поведении медицинского персонала.
Ошибки этого рода целиком относятся к
ошибкам деонтологического характера.
Говоря о проблеме врачебных ошибок
в целом И.А. Кассирский пишет:»
Врачебные ошибки — это серьезная и
всегда актуальная проблема врачевания.
Надо признать, что как бы ни было хорошо
поставлено медицинское дело, нельзя
представить себе врача, уже имеющего
за плечами большой научно-практический
стаж, с прекрасной клинической школой,
очень внимательного и серьезного, —
который в своей деятельности мог бы
безошибочно определить любое заболевание
и столь же безошибочно лечить его,
делать идеальные операции… Ошибки —
неизбежные и печальные издержки врачебной
деятельности, ошибки — это всегда плохо,
и единственное оптимальное, что
вытекает из трагедии врачебных ошибок
это то, что они по диалектике вещей
учат и помогают тому, что бы их не было.
Они несут в существе своем науку о том,
как не ошибаться и виновен не тот врач,
кто допускает ошибку, а тот, кто не
свободен от трусости отстаивать ее «.
/ Кассирский И.А. » О врачевании »
— М. Медицина. 1970 С.- 27 /.
Из сказанного можно выделить два
важных положения. Во-первых, признание
того, что врачебные ошибки неизбежны
во врачебной деятельности, поскольку
они вызываются не только субъективными
но и объективными причинами. И, во-вторых,
каждая врачебная ошибка должна
анализироваться и изучаться с тем, чтобы
она сама стала источником предупреждения
других ошибок. В нашей стране разработана
и применяется система анализа врачебных
действий вообще и врачебных ошибок в
частности, в форме клинико-анатомических
конференций.
Практика показывает, что в значительном
проценте случаев претензии к врачам и
среднему медицинскому персоналу
обусловлены, прежде всего, неправильным
поведением медицинского персонала по
отношению к больным, нарушением ими
деонтологических норм и правил.
Проанализируем, отмеченные выше
группы врачебных ошибок.
Диагностические ошибки.
Диагностические ошибки являются
самыми частыми. Формирование клинического
диагноза — весьма сложная и многокомпонентная
задача, решение которой основывается
с одной стороны, на знании врачом
этиологии, патогенеза, клинических и
патоморфологических проявлений
заболеваний и патологических процессов,
с другой стороны, на учете индивидуальных
особенностей их течения у данного
конкретного больного. Наиболее частой
причиной диагностических ошибок являются
ОБЪЕКТИВНЫЕ трудности, а иногда и
невозможность ранней диагностики
заболевания.
Многие болезненные процессы имеют
длительное течение со значительным по
времени латентным периодом, и
практически, бессимптомным течением.
Это относится к злокачественным
новообразованиям, хроническим отравлениям
и.т.п.
Большие диагностические трудности
возникают и при молниеносном течении
болезней. Как указывалось, объективными
причинами врачебных ошибок могут быть
атипичное течение заболевания или
комбинированные конкурирующие
заболевания, тяжелое состояние больного
при недостаточном на обследование
времени. Значительно затрудняет
диагностику алкогольное опьянение
больного, которое может маскировать
или извращать симптоматику заболевания
или травмы.
Причинами диагностических ошибок
могут быть недооценка или переоценка
анамнестических данных, жалоб больного,
результатов лабораторных и инструментальных
методов исследований. Однако эти причины
нельзя рассматривать как объективные,
ибо они упираются в недостаток
квалификации и опыта врача.
Приведу примеры некоторых диагностических
ошибок:
— У мальчика 10 лет появились боли в
животе, тошнота, повторная рвота, жидкий
водянистый стул. На другой день в каловых
массах появилась примесь слизи,
температура тела повысилась до 38 град.
Начало заболевания родители и мальчик
связывали с приемом пищи в столовой.
Через два дня ребенок был госпитализирован.
Предъявлял жалобы на разлитые боли в
животе. При осмотре отмечено, что живот
несколько напряжен, отмечается
болезненность во всех отделах. Признаки
раздражения брюшины отсутствуют. После
стула живот стал мягче, боли
локализовались по ходу восходящего и
нисходящего отделов кишечника. В крови
лейкоцитоз / 16 500 / СОЭ- 155 мм / час.
Выставлен диагноз:- острый
гастроэнтерит. Назначено консервативное
лечение. В дальнейшем состояние мальчика
не улучшилось. На третий день стационарного
лечения мальчик был осмотрен хирургом,
который исключил острые хирургические
заболевания, однако на следующий день
предложил перевести мальчика в
хирургическое отделение. Состояние
ребенка ухудшилось, появились признаки
перитонита. Произведена лапаротомия.
В брюшной полости обнаружен жидкий
гной. Источником перитонита оказался
гангренозно измененный аппендикс,
расположенный в полости малого таза,
в инфильтрате между слепой и сигмовидной
кишками. Спасти мальчика не удалось. По
заключению судебно-медицинской экспертной
комиссии причиной поздней диагностики
аппендицита явилось его атипичное
течение, обусловленное необычным
расположением червеобразного отростка
в полости малого таза.
В другом случае у женщины 76 лет
флегманозный аппендицит с инфильтрацией
окружающих тканей был ошибочно принят
за раковую опухоль слепой кишки. Этому
во многом способствовало атипичное
подострое течение болезни, повторные
рвоты, похудание больной, отсутствие
характерных симптомов раздражения
брюшины, при наличии четко определяемого
пальпаторно опухолевидного образования
в правой подвздошной области и явлений
кишечной непроходимости. Женщину
оперировали дважды. Первая операция —
паллиативная » формирование илиостомы
» Вторая радикальная — резекция толстой
кишки. Правильный диагноз был установлен
после исследования биопсийного материала
и на основании данных секционного
материала т.к. больная погибла в
результате сепсиса, явившегося осложнением
высокотравматичной операции.
Данный пример приведен как пример,
диагностической ошибки. Однако, при
более серьезном подходе здесь можно
обнаружить нарушение действующих
инструкций — в частности, больную нельзя
было брать на операцию без данных биопсии
т.к. состояние пациентки позволяло не
брать ее на операционный стол в экстренном
порядке. То есть в данном случае можно
было бы говорить об имевшем место,
врачебном преступлении. Категория
проступка не подходит т.к. ошибка
диагностики повлекла тяжкое последствие
— смерть.
Соседние файлы в папке Pravo
- #
- #
- #
- #
- #
- #
- #
- #
- #
Все чаще врачебная ошибка становится причиной возбуждения уголовных дел против врачей. Количество разбирательств увеличивается, но означает ли это, что ответственность за врачебную ошибку должна ужесточаться?
Как отдельный состав врачебная ошибка статья УК РФ в действующей редакции отсутствует, но обычно врачебная ошибка квалифицируется как непреднамеренные действия врача, которые совершаются в его профессиональной деятельности и влекут за собой неблагоприятные для пациента последствия.
Виды врачебных ошибок можно классифицировать, исходя из следующих факторов:
- Недостаточный профессионализм специалиста.
- Применение устаревших методов лечения и обследования больных.
- Несовершенство современной медицинской науки.
- Неблагоприятные условия в работе специалиста.
Как мы уже сказали, отдельной категории врачебная ошибка УК РФ и другие действующие законы не содержат. Однако, он распространён в тех случаях, когда необходимо определить содержание нарушений, происходящих при оказании медпомощи.
Именно эти причины врачебных ошибок лежат в основе классификации.
Классификация врачебных ошибок
Существуют разные врачебные ошибки, причины возникновения, классификация ошибок традиционно включает в себя следующие виды ошибочных действий врачей:
- технические ошибки – связаны с неверным применением лекарственных средств, методик диагностики, а также с неправильным применением медицинского оборудования, которое имеется в распоряжении врача;
- ошибки тактического характера – имеют место в том случае, если врач неверно выбрал объем вмешательств, выделил неправильные показания к медицинскому вмешательству, неверно выбрал время для процедур и т.д.;
- диагностическая врачебная ошибка – связана с ошибкой врача в диагнозе пациента, а также в нераспозновании имеющегося заболевания или состояния.
Ответственность в УК РФ за врачебные ошибки
В действующем УК РФ, врачебная ошибка статья отсутствует, однако, дела против медработников продолжают возбуждаться по другим составам – чаще всего по ст. 238 УК и ст. 109 УК РФ, которые выделяют разные составы преступлений:
- ч. 2 ст. 109 УК РФ определяется как некачественное медобслуживание пациента, которое привели к летальному исходу больного. В этом случае свободу врача могут по решению суда ограничить до 3-х лет, также специалиста могут принудить к обязательным работам. Право занимать определенные должности врачу могут ограничить до 3-х лет;
- ч. 2 ст. 238 УК РФ (врачебная ошибка статья УК). Статья предусматривает более строгие санкции в том случае, если вина врача будет доказана следствием. Так, врачебная ошибка может привести к 6 годам лишения свободы, к 5 годам принудительных работ, также возможны серьезные штрафные санкции – до 500 тысяч рублей. Наказание следует за виновные действия врача, которые привели к причинению тяжкого вреда здоровью пациента, либо к его смерти;
- ч. 3 238 УК РФ. Доказанная врачебная ошибка по данной статье может стоить специалисту 10 лет лишения свободы или 5 лет принудительных работ.
Какая ответственность за врачебную ошибку будет применена в конкретном случае законом определено. Случаи из судебной практики показывают, что к виновному может быть применена любая из этих статей, единых правил нет.
Возбуждение уголовного дела
Если была совершена врачебная ошибка, которая повлекла за собой тяжелые неблагоприятные последствия, события в дальнейшем развиваются по примерно одинаковому сценарию:
- Сам пациент или родственники погибшего пациента обращаются в следственные органы и прокуратуру с соответствующим заявлением. Нередко они обращаются и в само медицинское учреждение, требуя разбирательства по поводу врача, допустившего, по их мнению, халатность в своей работе.
- Возбуждению уголовного дела предшествует доследственная проверка. Эти занимаются дознаватели ил следователи, которые могут взять объяснения с самого медицинского работника, а также с его непосредственного руководителя.
Во многих случаях главный врач медучреждения даже не знает о том, что в отношении его сотрудника проводится доследственная проверка – следователи не обязаны ему об этом сообщать.
Более того, сам специалист, который допустил ошибку при выполнении своих профессиональных обязанностей может не знать о том, что пациент или его родные обратились в органы. Он узнает об этом только в том случае, если будет возбуждено уголовное дело.
- По итогам проверки в возбуждении дела могут отказать, второй вариант – возбуждение уголовного дела, что является довольно серьезным мероприятием для врача. В таком случае врач должен немедленно ознакомиться с постановлением следователя, где написано, по каким основаниям и по какому составу врачебная ошибка статья УК было возбуждено разбирательства
Можно ли повернуть процесс вспять, если дело уже завели
Однако, даже если уголовное дело по составам врачебной ошибки все же было возбуждено, оно может быть прекращено.
Для этого необходимо соблюдение двух условий:
- Преступление относится к категории дел небольшой или средней тяжести.
- Сам врач должен признать свое добросовестное заблуждение, примириться с потерпевшей стороной и загладить причиненный ей вред.
Например, ч. 2 т. 109 УК РФ отнесена именно к преступлениям средней тяжести. Это значит, что медработник, который впервые обвиняется в подобном преступлении, может быть освобожден от дальнейшего преследования.
Однако, даже если он совершит все необходимые действия, признает, что им была совершена врачебная ошибка, но вторая сторона категорически не согласиться с этим – дело уйдет в суд.
Судья также поинтересуется у потерпевшего, настаивает ли он на самом строгом наказании. Если пациент признает, что не настаивает, а врач возместил ему причиненные убытки и компенсировал моральный вред, то приговор суда будет не самым строгим.
Врачебная ошибка статья УК РФ 238 – относится к категории тяжких дел. Это значит, что даже примирение сторон не повлечет за собой прекращение уголовного дела.
Поэтому задача адвоката врача – постараться изменить квалификацию ст. 238 на ст. 109 УК РФ. Это даст возможность примириться с пациентом и избежать обвинительного приговора.
Особый порядок рассмотрения дел о «врачебных ошибках»
Ответственность за врачебную ошибку всегда рассматривается в уголовном процессе. Почему все чаще сторонам предлагают рассмотреть дело в особом порядке, и что это значит?
Особый порядок – это особая, упрощенная форма уголовного разбирательства. В этом случае врач признает свою вину, врачебная ошибка статья УК РФ, которая была ему вменена, а суд не проводит такие процедуры, как допрос свидетелей, исследование доказательств и их оценка.
Врачи часто соглашаются на этот вариант, т.к. чаще всего они просто морально устают от длительной процедуры расследования. При этом многие из них не понимают, какие последствия для них наступают после принятия такого решения.
Когда уголовное дело рассматривают в особом порядке
Заявить о рассмотрении дела в особом порядке обвиняемый может в тот момент, когда следователь предлагает ему ознакомиться с материалами уголовного дела. Для этого он подает соответствующее ходатайство.
Врач, которому вменяется врачебная ошибка должен понимать процессуальные последствия такого решения, их ему разъясняет следователь.
Для рассмотрения дела в особом порядке должны быть соблюдены следующие условия:
- Врач признает причинение вреда и полностью согласен с обвинением следствия.
- Обвиняемым заявлено ходатайство в период, который определен ст. 315 УПК РФ.
- Последствия и их характер осознаются обвиняемым.
- Прокурор не возражает против удовлетворения ходатайства обвиняемого.
- Врачу предъявлено обвинение, наказание по которому не превышает 10 лет лишения свободы.
- В ходе проведенного расследования было собрано достаточно доказательств, подтверждающих вину врача. Отсутствуют основания, по которому уголовное дело может быть прекращено.
Таким образом, если была совершена врачебная ошибка, которую врач понимает и признает, он при соблюдении данных условий может согласиться на особый порядок рассмотрения дела.

В какой-то момент при написании этого текста у меня проскочила мысль о том, что выбор темы — моя ошибка. Для медицинского сообщества эта тема болезненная. С одной стороны, у каждого из нас нашлось бы некоторое количество историй, когда диагноз пациенту был поставлен неверно или с опозданием. С другой стороны, все мы знаем, что так или иначе для всех виноват будет именно лечащий врач. Однако так ли это? Давайте поговорим о наших ошибках, основываясь на теоретических знаниях когнитивной психологии, системной инженерии и эргономики (научной дисциплины, изучающей взаимодействие человека и других элементов системы, а также сферы деятельности по применению теории, принципов, данных и методов этой науки для обеспечения благополучия человека и оптимизации общей производительности системы).
Упущенная возможность
 Юлия ПиневичДиагностическая ошибка сегодня — одна из важнейших проблем безопасности в здравоохранении. Признавая особую значимость этой проблемы, в 2015 году Национальная академия наук, инженерии и медицины США (NASEM) выпустила доклад «Улучшение диагностики в медицине». Согласно ему, диагностическая ошибка определяется как «неспособность дать точное и своевременное объяснение проблем со здоровьем пациента или неспособность сообщить об этом пациенту».
Юлия ПиневичДиагностическая ошибка сегодня — одна из важнейших проблем безопасности в здравоохранении. Признавая особую значимость этой проблемы, в 2015 году Национальная академия наук, инженерии и медицины США (NASEM) выпустила доклад «Улучшение диагностики в медицине». Согласно ему, диагностическая ошибка определяется как «неспособность дать точное и своевременное объяснение проблем со здоровьем пациента или неспособность сообщить об этом пациенту».
Другими словами, диагностическая ошибка — это «упущенная возможность поставить своевременный или правильный диагноз либо предпринять следующий шаг для установления диагноза на основании имеющихся на тот момент данных».
В результате диагностических ошибок необходимая терапия может быть отложена или вообще не назначена. Одновременно может быть начато неправильное/ненужное лечение. По некоторым оценкам, для терапевтов частота диагностических ошибок составляет от 10 % до 15 %. К сожалению, эти ошибки приводят к значительной заболеваемости и смертности пациентов.
Диагностические ошибки, ведущие к причинению вреда, чаще всего связаны с «большой тройкой»: диагнозами рака, сердечно-сосудистых или инфекционных заболеваний.
Причем заметьте, в топе пропущенных или несвоевременно установленных диагнозов часто встречающиеся колоректальный рак, рак легкого или рак молочной железы, инфаркт миокарда, инсульт, сепсис — совсем не карциноидная опухоль, системная красная волчанка, пароксизмальная ночная гемоглобинурия или криптококкоз. Помимо потенциальных неблагоприятных событий для пациента диагностические ошибки влекут за собой увеличение расходов в системе здравоохранения из-за избыточных диагностических тестов, менее эффективного и более дорогостоящего лечения.
Анализ проблемы
Прежде чем предложить те или иные пути решения любой проблемы, ее необходимо не только определить, но и измерить, описать в конкретных цифрах. Например, в одном французском медицинском центре были проанализированы ошибки при назначении лекарственных средств. Частота таких ошибок в ортопедическом отделении составила 30 %. После внедрения компьютеризированной системы для врачебных назначений таких ошибок стало в разы меньше — 2,4 %.
Инциденты, связанные с ошибками при назначении лекарственных средств, легко поддаются анализу. Это же касается и хирургических ошибок (выбор места оперативного вмешательства, повреждение органов и тканей, «забытые» инструменты и другие инородные тела), которые, как правило, всем очевидны. Все сложнее с диагностическими ошибками. Уровень диагностических ошибок чрезвычайно трудно измерить. Вскрытие, может, и покажет.
Согласно опубликованному систематическому обзору данных аутопсий, в 9 % случаев были выявлены серьез-ные диагностические ошибки, которые остались незамеченными прижизненно.
Но большинство ошибок, к счастью, не приводят к летальному исходу. Нередко точный диагноз устанавливается при повторном обращении пациента за помощью, в другом лечебном учреждении или другим врачом-специалистом. Медперсонал, который оказывал помощь при первичном контакте, остается в неведении, были ли допущены ошибки в диагностическом процессе. Да и как часто у нас есть возможность и желание проводить «когнитивную аутопсию» наших решений?
Когнитивные ошибки
Когнитивная психология изучает то, как человек обрабатывает информацию и впоследствии принимает решения. Для постановки предварительного диагноза, особенно когда мы сталкиваемся с типичными проявлениями заболевания, мы склонны использовать эвристики, или эмпирические правила.
Наши знания, прежний опыт, то, что еще называют профессиональной интуицией, позволяют нам использовать «короткий мыслительный путь»/быстрые суждения, что почти не требует усилий и временных затрат. Эти мыслительные приемы значительно облегчают решение ежедневных практических задач, позволяют быстро получить приблизительный результат, в типичных ситуациях этот результат близок к точному.
Если в приемном отделении мы осматриваем пациента с ангинозной болью, ишемическими изменениями на электрокардиограмме и положительными кардиоспецифическими маркерами, мы вряд ли ошибемся, если диагностируем острый коронарный синдром, а затем и инфаркт миокарда. Мы «узнаем» диагноз автоматически, не осознавая собственный мыслительный процесс.
Такая способность мозга значительно увеличивает нашу продуктивность. Проблема в том, что неправильное применение эвристик нередко приводит к диагностическим ошибкам (см. табл. 1). В абсолютном большинстве случаев мы будем правы с диагнозом инфаркта миокарда, но у одного пациента из ста кардиоспецифические маркеры не нарастают в динамике, присутствует асимметрия пульса, а вовремя выполненная эхокардиография выявит расслаивающуюся аневризму аорты.
Таблица 1. Неправильное применение эвристик, приводящее к ошибкам.
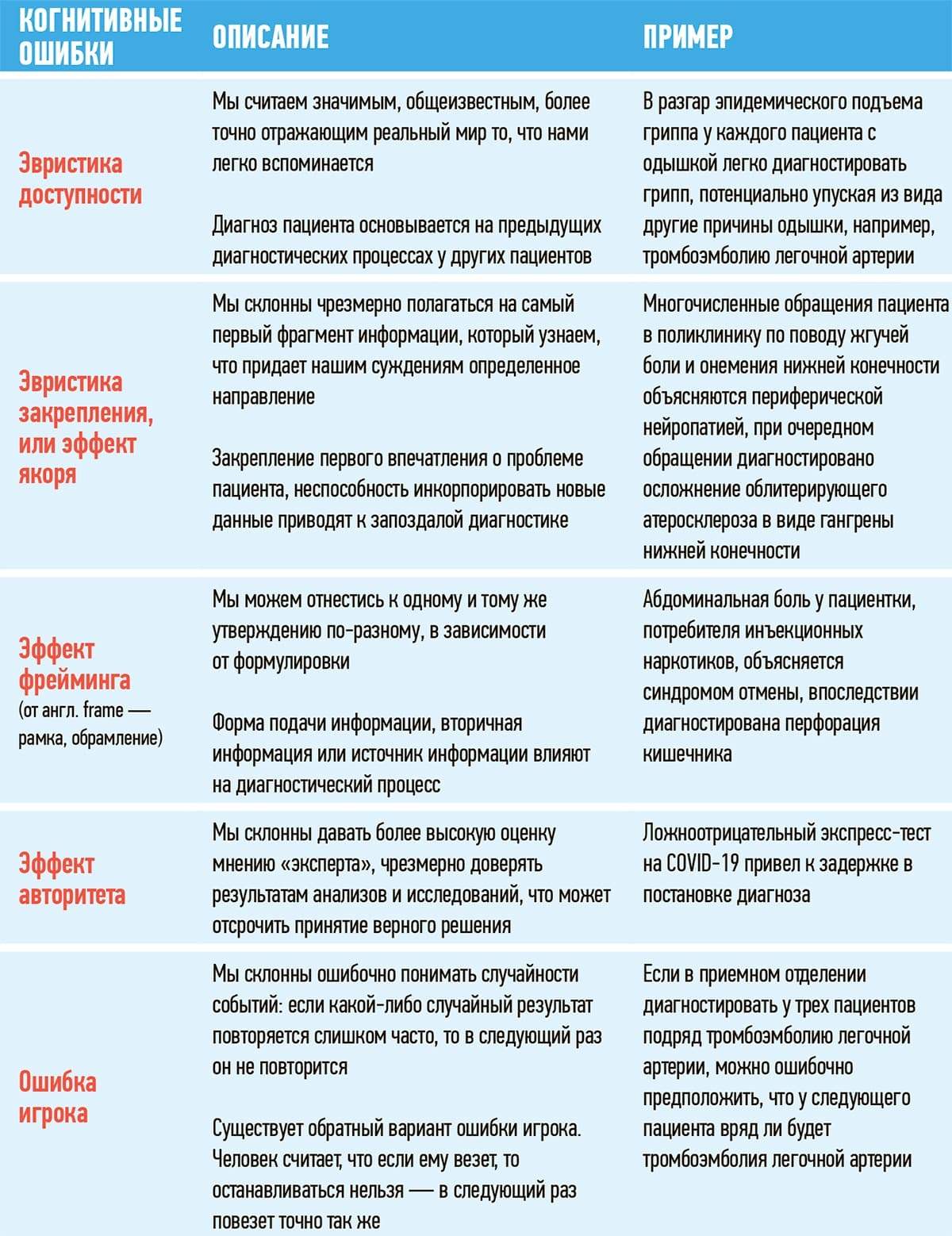
В таблице 1 приведены лишь основные примеры когнитивных искажений, которым мы все без исключения подвержены.
Есть еще одно особое когнитивное искажение — знание задним числом. На клинических разборах нам часто кажется, что установленный диагноз был очевиден с самого начала, что история текущего заболевания была вполне предсказуемой или даже неизбежной.
Когда мы знаем результат заранее, то склонны значительно переоценивать его предсказуемость или очевидность в сравнении с оценками тех, кто не знает, как развивались события. Стоит признать, что причинами наших ошибок может быть дефицит знаний как таковой, но все же несоизмеримо чаще наше клиническое мышление дает сбой.
Название одной из первых статей на эту тему из далекого 1998 года было интригующим: «Почему я упустил верный диагноз?» В статье был очень простой и точный ответ: «Я не думал о нем».
Системные факторы
Есть расхожее мнение, что основная причина неверных диагнозов — когнитивные ошибки врача. Такое утверждение является следствием упрощенного понимания не только проблемы диагностических ошибок, но и лечебно-диагностического процесса в целом. Диагностика — динамический процесс, который растянут во времени (вплоть до оценки эффективности назначенной терапии), а иногда и в пространстве.
Этот процесс включает взаимодействие между несколькими участниками: пациентом, врачами разных специальностей, сестринским персоналом, лаборантами, администрацией. Другой принципиально важный участник в этом процессе — технологии (оборудование, информационные системы, история болезни).
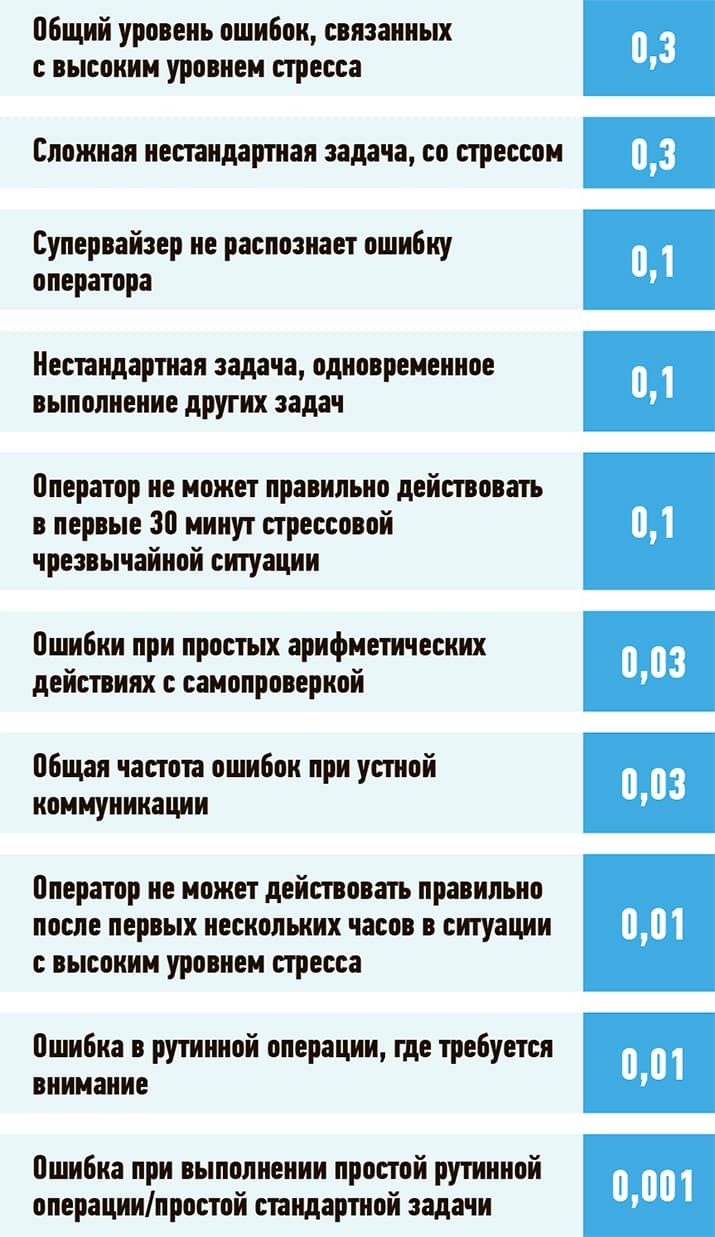
Человек — часть социотехнической системы, постоянно с ней взаимодействует при выполнении своих профессиональных обязанностей в разных областях: на производстве, в авиации, ядерной энергетике или медицине. Всем нам свойственно принимать ошибочные решения и в повседневной жизни, и в профессиональной. К слову, при выполнении стандартной повторяющейся задачи на производстве вероятность ошибки относительно невелика — от 0,1 % до 1 %. При выполнении нескольких задач одновременно вероятность ошибки составляет 10 %, а при выполнении сложной нестандартной задачи, особенно в условиях стресса, вероятность ошибиться возрастает до 30 % (см. табл. 2).
Таблица 2. Вероятность ошибки, связанной с человеческим фактором, на производстве.
Медицина ставит перед нами сложные задачи. На сегодняшний день известно о более 10 000 болезней и более 3 500 диагностических тестов, но сравнительно небольшое количество симптомов.
Таким образом, у любого одного симптома могут быть десятки, если не сотни возможных причин и вариантов верификации диагноза. Система здравоохранения связывает воедино сотни и тысячи людей, технологий и процессов (см. рис. 1). Огромное количество взаимо-связей между элементами системы увеличивает риск неправильной коммуникации и других сбоев в системе.
Рисунок 1. Основанная на принципах системной инженерии и эргономики SEIPS 2.0 модель, описывающая рабочую систему из взаимодействующих структурных элементов.
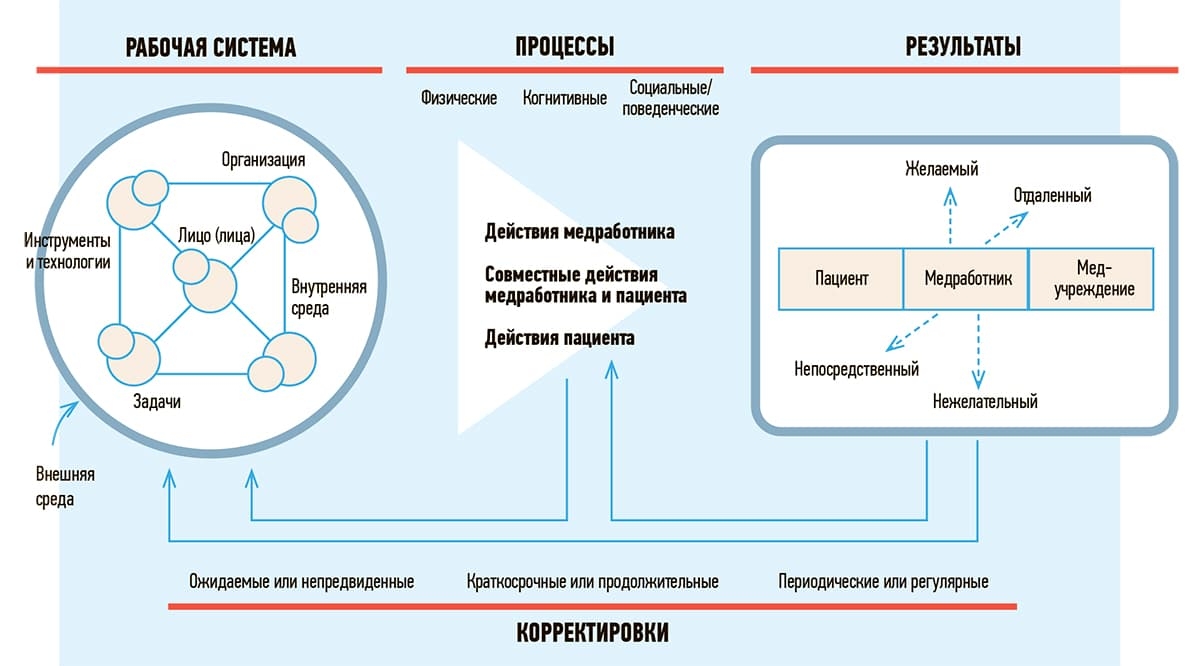
SEIPS описывает, как многочисленные взаимодействия между компонентами системы ведут к рабочим процессам, которые могут привести к различным результатам, включая непредвиденный.
К компонентам рабочей системы относят: 1) лицо (лица) — люди, работающие в системе, и па-циент; 2) задачи, выполняемые лицами, которые могут различаться по сложности или разнооб-разию; 3) инструменты и технологии — используются для выполнения задач, которые могут различаться по удобству использования и функциональности; 4) внутренняя среда — пространство вокруг людей, т. е. компоновка, шум, температура; 5) организация — условия, ресурсы и деятельность внутри организации; 6) внешняя среда — факторы за пределами учреждений здравоохранения, которые могут включать политические, социальные или экономические составляющие.
Процессы могут быть физическими, когнитивными или поведенческими и приводить к результа-там для пациентов (безопасность и эффективность лечения), медработников (удовлетворенность трудом, высокая профессиональная мотивация или эмоциональное выгорание) или медицинских учреждений (текучесть кадров).
Взаимодействия между компонентами рабочей системы приводят к разным результатам, поло-жительным и отрицательным. Структура включает в себя циклы обратной связи, представляю-щие корректировки, вносимые системами с течением времени.
По данным Объединенной комиссии (некоммерческая организация, занимающаяся аккредитацией медицинских организаций в США), 80 % серьезных медицинских ошибок связаны с дефектами коммуникации между медработниками во время передачи пациента от одного клинициста другому. Стресс, нехватка времени и персонала увеличивают риск ошибочного решения.
Вы когда-нибудь слышали что-то вроде: «я не собирался садиться нетрезвым за руль, но сел»? В таком случае еще можно с натяжкой предположить, что от ситуации, где все хорошо, до ситуации «катастрофа» — один неверный шаг. Модели причин катастроф, которые используются в инженерии, авиации и медицине, показывают, что у нас есть несколько уровней защиты от несчастных случаев и что только множественные сбои, просчеты при определенных условиях могут привести к катастрофе. Диагностическая ошибка чаще всего является следствием реализации сразу нескольких факторов, когнитивных и системных.
Одна из аналогий, которая используется для описания этого явления, — модель швейцарского сыра (см. рис. 2), разработанная психологом Джеймсом Ризоном в 1990 году. В этой модели компонент диагностического процесса будет представлять собой ломтик сыра в стопке ломтиков. У каждого компонента в процессе диагностики есть уязвимые места (представленные дырками в ломтике швейцарского сыра).
Рисунок 2. Модель швейцарского сыра Джеймса Ризона с модификациями.

Ломтики сыра — защитные барьеры. Дырки в сыре — прорехи из-за активных ошибок и латентных факторов.
На одном этапе диагностического процесса это может не повлиять на результат. Однако если уязвимости (дырки в швейцарском сыре) совпадут, может возникнуть диагностическая ошибка. Стоит ли говорить, что цена ошибки в нашей работе чрезвычайно высока? Чем выше устойчивость самой системы, тем меньше вероятность допустить ошибку, тем выше вероятность предотвратить негативные последствия такого инцидента (прежде всего вред пациенту) посредством раннего выявления и своевременных активных действий.
Когда мы пытаемся отрефлексировать причины диагностической ошибки, часто основное внимание уделяется выявлению неверного действия врача, в то время как остальные «дырки в сыре» — те самые латентные системные факторы — не замечаются. Следовательно, вероятность повторения такой ошибки в будущем остается высокой.
Выводы
Что со всем этим делать? Нет одного ответа. Профессиональное обучение, симуляционные тренинги, отработка коммуникативных навыков, внедрение чек-листов (например, в условиях, где высока вероятность систематических ошибок при выполнении рутинных действий), автоматизация рабочих процессов и поддержка диагностики с помощью компьютерных решений…
Но все это не будет работать, если «культура съест стратегию на завтрак».
Для начала необходимо принять тот факт, что как медработники мы подвержены тем же когнитивным ограничениям и предубеждениям, которые влияют на всех людей в повседневной жизни. Но это не значит, что мы снимаем с себя ответственность за неверное решение.
Важно создавать в коллективах атмосферу, в которой можно без колебаний сказать: «я не знаю» или «я ошибся».
Контроль качества и безопасность медицинской деятельности подразумевают создание безопасной для пациента и медработника среды, в которой процессы медицинской помощи проактивно анализируются для выявления дефектов или отклонений от стандартов. В такой среде медработник может высказать опасения по поводу недостатков медицинской помощи, которые могут привести к ошибкам в будущем. В этом и разница между виной и ответственностью.
A medical error is a preventable adverse effect of care («iatrogenesis»), whether or not it is evident or harmful to the patient. This might include an inaccurate or incomplete diagnosis or treatment of a disease, injury, syndrome, behavior, infection, or other ailment.
Definitions[edit]
The word error in medicine is used as a label for nearly all of the clinical incidents that harm patients. Medical errors are often described as human preventable errors in healthcare.[1] Whether the label is a medical error or human error, one definition used in medicine says that it occurs when a healthcare provider chooses an inappropriate method of care, improperly executes an appropriate method of care, or reads the wrong CT scan. It has been said that the definition should be the subject of more debate. For instance, studies of hand hygiene compliance of physicians in an ICU show that compliance varied from 19% to 85%.[2][needs update] The deaths that result from infections caught as a result of treatment providers improperly executing an appropriate method of care by not complying with known safety standards for hand hygiene are difficult to regard as innocent accidents or mistakes.
There are many types of medical error, from minor to major,[3] and causality is often poorly determined.[4][needs update]
There are many taxonomies for classifying medical errors.[5]
Definitions of diagnostic error[edit]
There is no single definition of diagnostic error, reflecting in part the dual nature of the word diagnosis, which is both a noun (the name of the assigned disease; diagnosis is a label) and a verb (the act of arriving at a diagnosis; diagnosis is a process). At the present time, there are at least 4 definitions of diagnostic error in active use:
Graber et al. defined diagnostic error as a diagnosis that is wrong, egregiously delayed, or missed altogether.[6] This is a ‘label’ definition, and can only be applied in retrospect, using some gold standard (for example, autopsy findings or a definitive laboratory test) to confirm the correct diagnosis. Many diagnostic errors fit several of these criteria; the categories overlap.
There are two process-related definitions: Schiff et al. defined diagnostic error as any breakdown in the diagnostic process, including both errors of omission and errors of commission.[7] Similarly, Singh et al. defined diagnostic error as a ‘missed opportunity’ in the diagnostic process, based on retrospective review.[8]
In its landmark report, Improving Diagnosis in Health Care, The National Academy of Medicine proposed a new, hybrid definition that includes both label- and process-related aspects: «A diagnostic error is failure to establish an accurate and timely explanation of the patient’s health problem(s) or to communicate that explanation to the patient.»[9] This is the only definition that specifically includes the patient in the definition wording.
Definition of prescription error[edit]
A prescription or medication error, as defined by the National Coordinating Council for Medication Error Reporting and Prevention, is an event that is preventable that leads to or has led to unsuitable use of medication or has led to harm to the person during the period of time that the medicine is controlled by a clinician, the person, or the consumer.[10] Some adverse drug events can also be related to medication errors.[11]
Impact[edit]
Medical errors affect one in 10 patients worldwide.[citation needed] One extrapolation suggests that 180,000 people die each year partly as a result of iatrogenic injury.[12] The World Health Organization registered 14 million new cases and 8.2 million cancer-related deaths in 2012. It estimated that the number of cases could increase by 70% through 2032. As the number of cancer patients receiving treatment increases, hospitals around the world are seeking ways to improve patient safety, to emphasize traceability and raise efficiency in their cancer treatment processes.[13] Children are often more vulnerable to a negative outcome when a medication error occurs as they have age-related differences in how their bodies absorb, metabolize, and excrete pharmaceutical agents.[14]
UK[edit]
In the UK, an estimated 850,000 medical errors occur each year, costing over £2 billion (estimated in the year 2000).[15] The accuracy of this estimate is not clear. Criticism has included the statistical handling of measurement errors in the report,[16] and significant subjectivity in determining which deaths were «avoidable» or due to medical error, and an erroneous assumption that 100% of patients would have survived if optimal care had been provided.[17]
A 2006 study found that medication errors are among the most common medical mistakes, harming at least 1.5 million people every year. According to the study, 400,000 preventable drug-related injuries occur each year in hospitals, 800,000 in long-term care settings, and roughly 530,000 among Medicare recipients in outpatient clinics. The report stated that these are likely to be conservative estimates. In 2000 alone, the extra medical costs incurred by preventable drug-related injuries approximated $887 million—and the study looked only at injuries sustained by Medicare recipients, a subset of clinic visitors. None of these figures take into account lost wages and productivity or other costs.[18]
US[edit]
According to a 2002 Agency for Healthcare Research and Quality report, about 7,000 people were estimated to die each year from medication errors – about 16 percent more deaths than the number attributable to work-related injuries (6,000 deaths).[citation needed] One in five Americans (22%) report that they or a family member have experienced a medical error of some kind.[19] A 2000 Institute of Medicine report estimated that medical errors result in between 44,000 and 98,000 preventable deaths and 1,000,000 excess injuries each year in U.S. hospitals.[20][21][22] A 2001 study in the Journal of the American Medical Association of seven Department of Veterans Affairs medical centers estimated that for roughly every 10,000 patients admitted to the select hospitals, one patient died who would have lived for three months or more in good cognitive health had «optimal» care been provided.[17] A 2001 study estimated that 1% of hospital admissions result in an adverse event due to negligence.[23] Identification or errors may be a challenge in these studies, and mistakes may be more common than reported as these studies identify only mistakes that led to measurable adverse events occurring soon after the errors. Independent review of doctors’ treatment plans suggests that decision-making could be improved in 14% of admissions; many of the benefits would have delayed manifestations.[24] Even this number may be an underestimate. One study suggests that adults in the United States receive only 55% of recommended care.[25] At the same time, a second study found that 30% of care in the United States may be unnecessary.[26] For example, if a doctor fails to order a mammogram that is past due, this mistake will not show up in the first type of study.[23] In addition, because no adverse event occurred during the short follow-up of the study, the mistake also would not show up in the second type of study[24] because only the principal treatment plans were critiqued. However, the mistake would be recorded in the third type of study. If a doctor recommends an unnecessary treatment or test, it may not show in any of these types of studies.
Cause of death on United States death certificates, statistically compiled by the Centers for Disease Control and Prevention (CDC), are coded in the International Classification of Disease (ICD), which does not include codes for human and system factors.[27][28]
Causes[edit]
The research literature showed that medical errors are caused by errors of commission and errors of omission.[29] Errors of omission are made when providers did not take action when they should have, while errors of commission occur when decisions and action are delayed.[29] Commission and omission errors have also been attributed with communication failures.[30][31]
Medical errors can be associated with inexperienced physicians and nurses, new procedures, extremes of age, and complex or urgent care.[32] Poor communication (whether in one’s own language or, as may be the case for medical tourists, another language), improper documentation, illegible handwriting, spelling errors, inadequate nurse-to-patient ratios, and similarly named medications are also known to contribute to the problem.[33][34] Misdiagnosis may be associated with individual characteristics of the patient or due to the patient multimorbidity.[35][36] Patient actions or inactions may also contribute significantly to medical errors.[31][30]
Healthcare complexity[edit]
Complicated technologies,[37][38] powerful drugs, intensive care, rare and multiple diseases,[39] and prolonged hospital stay can contribute to medical errors.[40] In turn, medical errors from carelessness or improper use of medical devices often lead to severe injuries or death. Since 2015, 60 injuries and 23 deaths have been caused by misplaced feeding tubes while using the Cortrak2 EAS system. The FDA recalled Avanos Medical’s Cortrak system in 2022 due to its severity and the high toll associated with the medical error.[41]
Complexity makes diagnosis especially challenging. There are less than 200 symptoms listed in Wikipedia,[42] but there are probably more than 10,000 known diseases. The World Health Organization’s system for the International Classification of Disease, 9th Edition from 1979 listed over 14,000 diagnosis codes.[43] Textbooks of medicine often describe the most typical presentations of a disease, but in many conditions patients may have variable presentations instead of the classical signs and symptoms. To add complexity, the signs and symptoms of a given condition change over time; in the early stages the signs and symptoms may be absent or minimal, and then these evolve as the condition progresses. Diagnosis is often challenging in infants and children who can’t clearly communicate their symptoms, and in the elderly, where signs and symptoms may be muted or absent.[44]
There are more than 7000 rare diseases alone, and in aggregate these are not uncommon: Roughly 1 in 17 patients will be diagnosed with a rare disease over their lifetime.[45] Physicians may have only learned a handful of these during their education and training.
System and process design[edit]
In 2000, The Institute of Medicine released «To Err is Human,» which asserted that the problem in medical errors is not bad people in health care—it is that good people are working in bad systems that need to be made safer.[20]
Poor communication and unclear lines of authority of physicians, nurses, and other care providers are also contributing factors.[46] Disconnected reporting systems within a hospital can result in fragmented systems in which numerous hand-offs of patients results in lack of coordination and errors.[47]
Other factors include the impression that action is being taken by other groups within the institution, reliance on automated systems to prevent error.,[48] and inadequate systems to share information about errors, which hampers analysis of contributory causes and improvement strategies.[49]
Cost-cutting measures by hospitals in response to reimbursement cutbacks can compromise patient safety.[50]
In emergencies, patient care may be rendered in areas poorly suited for safe monitoring. The American Institute of Architects has identified concerns for the safe design and construction of health care facilities.[51]
Infrastructure failure is also a concern. According to the WHO, 50% of medical equipment in developing countries is only partly usable due to lack of skilled operators or parts. As a result, diagnostic procedures or treatments cannot be performed, leading to substandard treatment.
The Joint Commission’s Annual Report on Quality and Safety 2007 found that inadequate communication between healthcare providers, or between providers and the patient and family members, was the root cause of over half the serious adverse events in accredited hospitals.[52] Other leading causes included inadequate assessment of the patient’s condition, and poor leadership or training.
Competency, education, and training[edit]
Variations in healthcare provider training & experience[46][53] and failure to acknowledge the prevalence and seriousness of medical errors also increase the risk.[54][55] The so-called July effect occurs when new residents arrive at teaching hospitals, causing an increase in medication errors according to a study of data from 1979 to 2006.[56][57]
Human factors and ergonomics[edit]

Cognitive errors commonly encountered in medicine were initially identified by psychologists Amos Tversky and Daniel Kahneman in the early 1970s. Jerome Groopman, author of How Doctors Think, says these are «cognitive pitfalls», biases which cloud our logic. For example, a practitioner may overvalue the first data encountered, skewing their thinking. Another example may be where the practitioner recalls a recent or dramatic case that quickly comes to mind, coloring the practitioner’s judgement. Another pitfall is where stereotypes may prejudice thinking.[58] Pat Croskerry describes clinical reasoning as an interplay between intuitive, subconscious thought (System 1) and deliberate, conscious rational consideration (System 2). In this framework, many cognitive errors reflect over-reliance on System 1 processing, although cognitive errors may also sometimes involve System 2.[59]
Sleep deprivation has also been cited as a contributing factor in medical errors.[60] One study found that being awake for over 24 hours caused medical interns to double or triple the number of preventable medical errors, including those that resulted in injury or death.[61] The risk of car crash after these shifts increased by 168%, and the risk of near miss by 460%.[62] Interns admitted falling asleep during lectures, during rounds, and even during surgeries.[62] Night shifts are associated with worse surgeon performance during laparoscopic surgeries.[60]
Practitioner risk factors include fatigue,[63][64][65]
depression,[66] and burnout.[67]
Factors related to the clinical setting include diverse patients, unfamiliar settings, time pressures, and increased patient-to-nurse staffing ratio increases.[68]
Drug names that look alike or sound alike are also a problem.[69]
Errors in interpreting medical images are often perceptual instead of «fact-based»; these errors are often caused by failures of attention or vision.[70] For example, visual illusions can cause radiologists to misperceive images.[71]
A number of Information Technology (IT) systems have been developed to detect and prevent medication errors, the most common type of medical errors.[72] These systems screen data such as ICD-9 codes, pharmacy and laboratory data. Rules are used to look for changes in medication orders, and abnormal laboratory results that may be indicative of medication errors and/or adverse drug events.[73]
Examples[edit]
Errors can include misdiagnosis or delayed diagnosis, administration of the wrong drug to the wrong patient or in the wrong way, giving multiple drugs that interact negatively, surgery on an incorrect site, failure to remove all surgical instruments, failure to take the correct blood type into account, or incorrect record-keeping. A 10th type of error is ones which are not watched for by researchers, such as RNs failing to program an IV pump to give a full dose of IV antibiotics or other medication.
Errors in diagnosis[edit]
According to a 2016 study from Johns Hopkins Medicine, medical errors are the third-leading cause of death in the United States.[74] The projected cost of these errors to the U.S. economy is approximately $20 billion, 87% of which are direct increases in medical costs of providing services to patient affected by medical errors.[75] Medical errors can increase average hospital costs by as much as $4,769 per patient.[76] One common type of medical error stems from x-rays and medical imaging: failing to see or notice signs of disease on an image.[70] The retrospective «miss» rate among abnormal imaging studies is reported to be as high as 30% (the real-life error rate is much lower, around 4-5%, because not all images are abnormal),[77] and up to 20% of missed findings result in long-term adverse effects.[78][79]
A large study reported several cases where patients were wrongly told that they were HIV-negative when the physicians erroneously ordered and interpreted HTLV (a closely related virus) testing rather than HIV testing. In the same study, >90% of HTLV tests were ordered erroneously.[80]
It is estimated[by whom?] that between 10 and 15% of physician diagnoses are erroneous.[81]
Misdiagnosis of lower extremity cellulitis is estimated to occur in 30% of patients, leading to unnecessary hospitalizations in 85% and unnecessary antibiotic use in 92%. Collectively, these errors lead to between 50,000 and 130,000 unnecessary hospitalizations and between $195 and $515 million in avoidable health care spending annually in the United States.[82]
Misdiagnosis of psychological disorders[edit]
Female sexual desire sometimes used to be diagnosed as female hysteria.[citation needed]
Sensitivities to foods and food allergies risk being misdiagnosed as the anxiety disorder orthorexia.
Studies have found that bipolar disorder has often been misdiagnosed as major depression. Its early diagnosis necessitates that clinicians pay attention to the features of the patient’s depression and also look for present or prior hypomanic or manic symptomatology.[83]
The misdiagnosis of schizophrenia is also a common problem. There may be long delays of patients getting a correct diagnosis of this disorder.[84]
Delayed sleep phase disorder is often confused with: psychophysiological insomnia; depression; psychiatric disorders such as schizophrenia, ADHD or ADD; other sleep disorders; or school refusal. Practitioners of sleep medicine point out the dismally low rate of accurate diagnosis of the disorder, and have often asked for better physician education on sleep disorders.[85]
Cluster headaches are often misdiagnosed, mismanaged, or undiagnosed for many years; they may be confused with migraine, «cluster-like» headache (or mimics), CH subtypes, other TACs ( trigeminal autonomic cephalalgias), or other types of primary or secondary headache syndrome.[86] Cluster-like head pain may be diagnosed as secondary headache rather than cluster headache.[87] Under-recognition of CH by health care professionals is reflected in consistent findings in Europe and the United States that the average time to diagnosis is around seven years.[88]
Asperger syndrome and autism tend to get undiagnosed or delayed recognition and delayed diagnosis[89][90] or misdiagnosed.[91] Delayed or mistaken diagnosis can be traumatic for individuals and families; for example, misdiagnosis can lead to medications that worsen behavior.[92][93]
The DSM-5 field trials included «test-retest reliability» which involved different clinicians doing independent evaluations of the same patient—a new approach to the study of diagnostic reliability.[94]
Outpatient vs. inpatient[edit]
Misdiagnosis is the leading cause of medical error in outpatient facilities.
Since the National Institute of Medicine’s 1999 report, «To Err is Human,» found up to 98,000 hospital patients die from preventable medical errors in the U.S. each year, government and private sector efforts have focused on inpatient safety.
Medical prescriptions[edit]
While in 2000 the Committee on Quality of Health Care in America affirmed medical mistakes are an «unavoidable outcome of learning to practice medicine»,[95] at 2019 the commonly accepted link between prescribing skills and clinical clerkships was not yet demonstrated by the available data[96] and in the U.S. legibility of handwritten prescriptions has been indirectly responsible for at least 7,000 deaths annually.[97]
Prescription errors concern ambiguous abbreviations, the right spelling of the full name of drugs: improper use of the nomenclature, of decimal points, unit or rate expressions; legibility and proper instructions; miscalculations of the posology (quantity, route and frequency of administration, duration of the treatment, dosage form and dosage strength); lack of information about patients (e.g. allergy, declining renal function) or reported in the medical document.[96] There were an estimated 66 million clinically significant medication errors in the British NHS in 2018. The resulting adverse drug reactions are estimated to cause around 700 deaths a year in England and to contribute to around 22,000 deaths a year. The British researchers did not find any evidence that error rates were lower in other countries, and the global cost was estimated at $42 billion per year.[98]
Medication errors in hospital include omissions, delayed dosing and incorrect medication administrations. Medication errors are not always readily identified, but can be reported using case note reviews or incident reporting systems.[99] There are pharmacist-led interventions that can reduce the incident of medication error.[100] Electronic prescribing has been shown to reduce prescribing errors by up to 30%.[101]
Mitigation (after an error)[edit]
Mistakes can have a strongly negative emotional impact on the doctors who commit them.[102][103][104][105]
Recognizing that mistakes are not isolated events[edit]
Some physicians recognize that adverse outcomes from errors usually do not happen because of an isolated error and actually reflect system problems.[53] This concept is often referred to as the Swiss Cheese Model.[106] This is the concept that there are layers of protection for clinicians and patients to prevent mistakes from occurring. Therefore, even if a doctor or nurse makes a small error (e.g. incorrect dose of drug written on a drug chart by doctor), this is picked up before it actually affects patient care (e.g. pharmacist checks the drug chart and rectifies the error).[106] Such mechanisms include:
Practical alterations (e.g.-medications that cannot be given through IV, are fitted with tubing which means they cannot be linked to an IV even if a clinician makes a mistake and tries to),[107] systematic safety processes (e.g. all patients must have a Waterlow score assessment and falls assessment completed on admission),[107] and training programmes/continuing professional development courses[107] are measures that may be put in place.
There may be several breakdowns in processes to allow one adverse outcome.[108] In addition, errors are more common when other demands compete for a physician’s attention.[109][110][111] However, placing too much blame on the system may not be constructive.[53]
Placing the practice of medicine in perspective[edit]
Essayists imply that the potential to make mistakes is part of what makes being a physician rewarding and without this potential the rewards of medical practice would be diminished. Laurence states that «Everybody dies, you and all of your patients. All relationships end. Would you want it any other way? […] Don’t take it personally»[112]
Seder states «[…] if I left medicine, I would mourn its loss as I’ve mourned the passage of my poetry. On a daily basis, it is both a privilege and a joy to have the trust of patients and their families and the camaraderie of peers. There is no challenge to make your blood race like that of a difficult case, no mind game as rigorous as the challenging differential diagnosis, and though the stakes are high, so are the rewards.»[113]
Disclosing mistakes[edit]
Forgiveness, which is part of many cultural traditions, may be important in coping with medical mistakes.[114] Among other healing processes, it can be accomplished through the use of communicative disclosure guidelines.[115]
To oneself[edit]
Inability to forgive oneself may create a cycle of distress and increased likelihood of a future error.[116]
However, Wu et al. suggest «…those who coped by accepting responsibility were more likely to make constructive changes in practice, but [also] to experience more emotional distress.»[117] It may be helpful to consider the much larger number of patients who are not exposed to mistakes and are helped by medical care.[113]
To patients[edit]
Gallagher et al. state that patients want «information about what happened, why the error happened, how the error’s consequences will be mitigated, and how recurrences will be prevented.»[118] Interviews with patients and families reported in a 2003 book by Rosemary Gibson and Janardan Prasad Singh, put forward that those who have been harmed by medical errors face a «wall of silence» and «want an acknowledgement» of the harm.[119] With honesty, «healing can begin not just for the patients and their families but also the doctors, nurses and others involved.» In a line of experimental investigations, Annegret Hannawa et al. developed evidence-based disclosure guidelines under the scientific «Medical Error Disclosure Competence (MEDC)» framework.[115][120]
A 2005 study by Wendy Levinson of the University of Toronto showed surgeons discussing medical errors used the word «error» or «mistake» in only 57 percent of disclosure conversations and offered a verbal apology only 47 percent of the time.[121]
Patient disclosure is important in the medical error process. The current standard of practice at many hospitals is to disclose errors to patients when they occur. In the past, it was a common fear that disclosure to the patient would incite a malpractice lawsuit. Many physicians would not explain that an error had taken place, causing a lack of trust toward the healthcare community. In 2007, 34 states passed legislation that precludes any information from a physician’s apology for a medical error from being used in malpractice court (even a full admission of fault).[122] This encourages physicians to acknowledge and explain mistakes to patients, keeping an open line of communication.
The American Medical Association’s Council on Ethical and Judicial Affairs states in its ethics code:
- «Situations occasionally occur in which a patient suffers significant medical complications that may have resulted from the physician’s mistake or judgment. In these situations, the physician is ethically required to inform the patient of all facts necessary to ensure understanding of what has occurred. Concern regarding legal liability which might result following truthful disclosure should not affect the physician’s honesty with a patient.»
From the American College of Physicians Ethics Manual:[123]
- «In addition, physicians should disclose to patients information about procedural or judgment errors made in the course of care if such information is material to the patient’s well-being. Errors do not necessarily constitute improper, negligent, or unethical behavior, but failure to disclose them may.»
However, «there appears to be a gap between physicians’ attitudes and practices regarding error disclosure. Willingness to disclose errors was associated with higher training level and a variety of patient-centered attitudes, and it was not lessened by previous exposure to malpractice litigation».[124] Hospital administrators may share these concerns.[125]
Consequently, in the United States, many states have enacted laws excluding expressions of sympathy after accidents as proof of liability.
Disclosure may actually reduce malpractice payments.[126][127]
To non-physicians[edit]
In a study of physicians who reported having made a mistake, it was offered that disclosing to non-physician sources of support may reduce stress more than disclosing to physician colleagues.[128] This may be due to the finding that of the physicians in the same study, when presented with a hypothetical scenario of a mistake made by another colleague, only 32% of them would have unconditionally offered support. It is possible that greater benefit occurs when spouses are physicians.[129]
To other physicians[edit]
Discussing mistakes with other physicians is beneficial.[53] However, medical providers may be less forgiving of one another.[129] The reason is not clear, but one essayist has admonished, «Don’t Take Too Much Joy in the Mistakes of Other Doctors.»[130]
To the physician’s institution[edit]
Disclosure of errors, especially ‘near misses’ may be able to reduce subsequent errors in institutions that are capable of reviewing near misses.[131] However, doctors report that institutions may not be supportive of the doctor.[53]
Use of rationalization to cover up medical errors[edit]
Based on anecdotal and survey evidence, Banja[132] states that rationalization (making excuses) is very common among the medical profession to cover up medical errors.
By potential for harm to the patient[edit]
In a survey of more than 10,000 physicians in the United States, when asked the question, «Are there times when it’s acceptable to cover up or avoid revealing a mistake if that mistake would not cause harm to the patient?», 19% answered yes, 60% answered no and 21% answered it depends. On the question, «Are there times when it is acceptable to cover up or avoid revealing a mistake if that mistake would potentially or likely harm the patient?», 2% answered yes, 95% answered no and 3% answered it depends.[133]
Legal procedure[edit]
Standards and regulations for medical malpractice vary by country and jurisdiction within countries. Medical professionals may obtain professional liability insurances to offset the risk and costs of lawsuits based on medical malpractice.
Prevention[edit]
Medical care is frequently compared adversely to aviation; while many of the factors that lead to errors in both fields are similar, aviation’s error management protocols are regarded as much more effective.[134] Safety measures include informed consent, the availability of a second practitioner’s opinion, voluntary reporting of errors, root cause analysis, reminders to improve patient medication adherence, hospital accreditation, and systems to ensure review by experienced or specialist practitioners.[135]
A template has been developed for the design (both structure and operation) of hospital medication safety programmes, particularly for acute tertiary settings,[136] which emphasizes safety culture, infrastructure, data (error detection and analysis), communication and training.
Particularly to prevent the medication errors in the perspective of the intrathecal administration of local anaesthetics, there is a proposal to change the presentation and packaging of the appliances and agents used for this purpose. One spinal needle with a syringe prefilled with the local anaesthetic agents may be marketed in a single blister pack, which will be peeled open and presented before the anaesthesiologist conducting the procedure.[137]
Physician well-being has also been recommended as an indicator of healthcare quality given its association with patient safety outcomes.[138] A meta-analysis involving 21517 participants found that physicians with depressive symptoms had a 95% higher risk of reporting medical errors and that the association between physician depressive symptoms and medical errors is bidirectional [66]
Reporting requirements[edit]
In the United States, adverse medical event reporting systems were mandated in just over half (27) of the states as of 2014, a figure unchanged since 2007.[139][140] In U.S. hospitals error reporting is a condition of payment by Medicare.[141] An investigation by the Office of Inspector General, Department of Health and Human Services released January 6, 2012 found that most errors are not reported and even in the case of errors that are reported and investigated changes are seldom made which would prevent them in the future. The investigation revealed that there was often lack of knowledge regarding which events were reportable and recommended that lists of reportable events be developed.[142]
Cause-specific preventive measures[edit]
Traditionally, errors are attributed to mistakes made by individuals, who then may be penalized. A common approach to respond to and prevent specific errors is requiring additional checks at particular points in the system, whose findings and detail of execution must be recorded. As an example, an error of free flow IV administration of heparin is approached by teaching staff how to use the IV systems and to use special care in setting the IV pump. While overall errors become less likely, the checks add to workload and may in themselves be a cause of additional errors. In some hospitals, a regular morbidity and mortality conference meeting is scheduled to discuss complications or deaths and learn from or improve the overall processes.
A newer model for improvement in medical care takes its origin from the work of W. Edwards Deming in a model of Total Quality Management.[citation needed] In this model, there is an attempt to identify the underlying system defect that allowed the error to occur. As an example, in such a system the error of free flow IV administration of heparin is dealt with by not using IV heparin and substituting subcutaneous administration of heparin, obviating the entire problem. However, such an approach presupposes available research showing that subcutaneous heparin is as effective as IV. Thus, most systems use a combination of approaches to the problem.[citation needed]
Anaesthesiology[edit]
The field of medicine that has taken the lead in systems approaches to safety is anaesthesiology.[143] Steps such as standardization of IV medications to 1 ml doses, national and international color-coding standards, and development of improved airway support devices has the field a model of systems improvement in care.
Medications[edit]
Reducing errors in prescribing, dispensing, compounding/formulating, labelling, and handling medications is a priority and has been the subject of systematic reviews and studies. Examples of areas to reduce medication errors and improve safety include: Training professionals or using databases to compare new and previous prescribed medications to prevent mistakes, also known as ‘medication reconciliation’,[144] prescribing through an electronic medical record system and/or using decision support systems that has automatic checks in place,with computerized alerts or other novel technologies, the use of machine-readable barcodes, healthcare professional and patient training or supplementary educational programs, adding in an extra step for double checking prescriptions (both at the level of the healthcare professional and at the administrator level), using standardized protocols in the workplace that include a check-list, physical markings or writing on syringes to indicate correct doses, programmes that include the person being able to administer the medications themselves, ensuring that the workplace or environment is well-lit, monitoring and adjusting healthcare professional working hours, and the use of an interdisciplinary team.[11] There is weak evidence indicating that a number of these suggested interventions may be helpful in reducing errors or improving patient safety, however, in general, evidence supporting the best or most effective intervention for reducing errors not strong.[11][145] Evidence supporting improvements aimed at reducing medical errors in medications for pediatric hospitalized patients is also very weak.[14]
Historically[edit]
As far back as the 1930s, pharmacists worked with physicians to select, from many options, the safest and most effective drugs available for use in hospitals.[146] The process is known as the Formulary System and the list of drugs is known as the Formulary. In the 1960s, hospitals implemented unit dose packaging and unit dose drug distribution systems to reduce the risk of wrong drug and wrong dose errors in hospitalized patients;[147] centralized sterile admixture services were shown to decrease the risks of contaminated and infected intravenous medications;[148][149] and pharmacists provided drug information and clinical decision support directly to physicians to improve the safe and effective use of medications.[150] Pharmacists are recognized experts in medication safety and have made many contributions that reduce error and improve patient care over the last 50 years. More recently, governments have attempted to address issues like patient-pharmacist communication and consumer knowledge through measures like the Australian Government’s Quality Use of Medicines policy.[citation needed]
Misconceptions[edit]
Some common misconceptions about medical error include:
- Medical error is the «third leading cause of death» in the United States. This canard stems from an erroneous 2016 study which, according to David Gorski, «has taken on a life of its own» and fuelled «a myth promulgated by both quacks and academics».[151]
- «Bad apples» or incompetent health care providers are a common cause. (Although human error is commonly an initiating event, the faulty care delivery process invariably permits or compounds the harm and so is the focus of improvement.)[22]
- High-risk procedures or medical specialties are responsible for most avoidable adverse events. (Although some mistakes, such as in surgery, are harder to conceal, errors occur in all levels of care.[22] Even though complex procedures entail more risk, adverse outcomes are not usually due to error, but to the severity of the condition being treated.)[46][152] However, United States Pharmacopeia has reported that medication errors during the course of a surgical procedure are three times more likely to cause harm to a patient than those occurring in other types of hospital care.[47]
- If a patient experiences an adverse event during the process of care, an error has occurred. (Most medical care entails some level of risk, and there can be complications or side effects, even unforeseen ones, from the underlying condition or from the treatment itself.)[20]
See also[edit]
- Serious adverse event
- Adverse drug reaction
- Biosafety
- Emily’s Law
- Fatal Care: Survive in the U.S. Health System (book)
- Medical malpractice
- Medical resident work hours
- Sleep deprivation
- Patient Safety and Quality Improvement Act of 2005
- Patient safety organization
- Quality Use of Medicines
References[edit]
- ^ Zhang J; Pate, VL; Johnson TR (2008). «Medical error: Is the solution medical or cognitive?». Journal of the American Medical Informatics Association. 6 (Supp1): 75–77. doi:10.1197/jamia.M1232. PMC 419424. PMID 12386188.
- ^ Salemi C, Canola MT, Eck EK (January 2002). «Hand washing and physicians: how to get them together». Infect Control Hosp Epidemiol. 23 (1): 32–5. doi:10.1086/501965. PMID 11868890. S2CID 18663388.
- ^ Hofer, TP; Kerr, EA; Hayward, RA (2000). «What is an error?». Effective Clinical Practice. 3 (6): 261–9. PMID 11151522. Archived from the original on September 28, 2007. Retrieved June 11, 2007.
- ^ Hayward, Rodney A.; Hofer, Timothy P. (July 25, 2001). «Estimating Hospital Deaths Due to Medical Errors: Preventability Is in the Eye of the Reviewer». JAMA. 286 (4): 415–20. doi:10.1001/jama.286.4.415. PMID 11466119.
- ^ Kopec, D.; Tamang, S.; Levy, K.; Eckhardt, R.; Shagas, G. (2006). «The state of the art in the reduction of medical errors». Studies in Health Technology and Informatics. 121: 126–37. PMID 17095810.
- ^ Graber ML, Franklin N, Gordon R. Diagnostic error in internal medicine. Arch Intern Med. 2005;165(13):1493-1499.
- ^ Schiff GD, Hasan O, Kim S, et al. Diagnostic Error in Medicine — Analysis of 583 Physician-Reported Errors. Arch Int Med. 2009;169(20):1881-1887.
- ^ Singh H. Helping health care organizations to define diagnostic errors as missed opportunities in diagnosis. Joint Commission Journal on Quality and Patient Safety. 2014;40(3):99-101.
- ^ Institute of Medicine. Improving Diagnosis in Health Care. National Academies Press, Washington, DC. 2015.
- ^ «Medication Error Definition». National Coordinating Council for Medication Error Reporting and Prevention. Retrieved July 17, 2023.
- ^ a b c Ciapponi, Agustín; Fernandez Nievas, Simon E; Seijo, Mariana; Rodríguez, María Belén; Vietto, Valeria; García-Perdomo, Herney A; Virgilio, Sacha; Fajreldines, Ana V; Tost, Josep; Rose, Christopher J; Garcia-Elorrio, Ezequiel (November 25, 2021). «Reducing medication errors for adults in hospital settings». Cochrane Database of Systematic Reviews. 2021 (11): CD009985. doi:10.1002/14651858.CD009985.pub2. PMC 8614640. PMID 34822165.
- ^ Leape LL (1994). «Error in medicine». JAMA. 272 (23): 1851–7. doi:10.1001/jama.272.23.1851. PMID 7503827.
- ^ «Cancer». World Health Organization. Retrieved March 2, 2017.
- ^ a b Maaskant, Jolanda M; Vermeulen, Hester; Apampa, Bugewa; Fernando, Bernard; Ghaleb, Maisoon A; Neubert, Antje; Thayyil, Sudhin; Soe, Aung (March 10, 2015). Cochrane Effective Practice and Organisation of Care Group (ed.). «Interventions for reducing medication errors in children in hospital». Cochrane Database of Systematic Reviews (3): CD006208. doi:10.1002/14651858.CD006208.pub3. PMID 25756542.
- ^ Donaldson, L (2000). «An organisation with a memory: Report of an expert group on learning from adverse events in the NHS». Patient Safety Network, UK. Retrieved July 17, 2023.
- ^ Hayward, Rodney A.; Heisler, Michele; Adams, John; Dudley, R. Adams; Hofer, Timothy P. (August 2007). «Overestimating Outcome Rates: Statistical Estimation When Reliability Is Suboptimal». Health Services Research. 42 (4): 1718–1738. doi:10.1111/j.1475-6773.2006.00661.x. PMC 1955272. PMID 17610445.
- ^ a b Hayward R, Hofer T (2001). «Estimating hospital deaths due to medical errors: preventability is in the eye of the reviewer». JAMA. 286 (4): 415–20. doi:10.1001/jama.286.4.415. PMID 11466119.
- ^ «Medication Errors Injure 1.5 Million People and Cost Billions of Dollars Annually». The National Academy of Science. 2006.
- ^ 2002 Annual Report Archived April 16, 2018, at the Wayback Machine, The Commonwealth Fund
- ^ a b c Institute of Medicine (2000). To Err Is Human: Building a Safer Health System. Washington, DC: The National Academies Press. p. 4. doi:10.17226/9728. ISBN 978-0-309-26174-6. PMID 25077248.
- ^ Charatan, Fred (March 4, 2000). «Clinton acts to reduce medical mistakes». BMJ. 320 (7235): 597. doi:10.1136/bmj.320.7235.597. PMC 1117638. PMID 10698861.
- ^ a b c Weingart SN, Wilson RM, Gibberd RW, Harrison B (March 2000). «Epidemiology of medical error». BMJ. 320 (7237): 774–7. doi:10.1136/bmj.320.7237.774. PMC 1117772. PMID 10720365.
- ^ a b Brennan T, Leape L, Laird N, Hebert L, Localio A, Lawthers A, Newhouse J, Weiler P, Hiatt H (1991). «Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I». N Engl J Med. 324 (6): 370–6. doi:10.1056/NEJM199102073240604. PMID 1987460. S2CID 3101439.
- ^ a b Lucas B, Evans A, Reilly B, Khodakov Y, Perumal K, Rohr L, Akamah J, Alausa T, Smith C, Smith J (2004). «The Impact of Evidence on Physicians’ Inpatient Treatment Decisions». J Gen Intern Med. 19 (5 Pt 1): 402–9. doi:10.1111/j.1525-1497.2004.30306.x. PMC 1492243. PMID 15109337.
- ^ McGlynn EA, Asch SM, Adams J, Keesey J, Hicks J, DeCristofaro A, Kerr EA (2003). «The quality of health care delivered to adults in the United States». N Engl J Med. 348 (26): 2635–45. doi:10.1056/NEJMsa022615. PMID 12826639.
- ^ Fisher ES (October 2003). «Medical Care — Is More Always Better?». New England Journal of Medicine. 349 (17): 1665–7. doi:10.1056/NEJMe038149. PMID 14573739.
- ^ Makary, Martin A; Daniel, Michael (May 3, 2016). «Medical error—the third leading cause of death in the US». BMJ. 353: i2139. doi:10.1136/bmj.i2139. PMID 27143499. S2CID 206910205.
- ^ Moriyama, IM; Loy, RM; Robb-Smith, AHT (2011). Rosenberg, HM; Hoyert, DL (eds.). History of the Statistical Classification of Diseases and Causes of Death (PDF). Hyattsville, MD: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics. ISBN 978-0-8406-0644-0.
- ^ a b Clapper, Timothy C.; Ching, Kevin (2020). «Debunking the myth that the majority of medical errors are attributed to communication». Medical Education. 54 (1): 74–81. doi:10.1111/medu.13821. ISSN 1365-2923. PMID 31509277.
- ^ a b Hannawa, Annegret; Wendt, Anne; Day, Lisa J. (December 4, 2017). New Horizons in Patient Safety: Safe Communication: Evidence-based core Competencies with Case Studies from Nursing Practice. De Gruyter. doi:10.1515/9783110454857. ISBN 978-3-11-045485-7.
- ^ a b Hannawa, Annegret; Wu, Albert; Juhasz, Robert (March 6, 2017). New Horizons in Patient Safety: Understanding Communication: Case Studies for Physicians. De Gruyter. doi:10.1515/9783110455014. ISBN 978-3-11-045501-4.
- ^ Harrison, Bernadette; Gibberd, Robert W.; Wilson, Ross McL; Weingart, N. Saul (March 18, 2000). «Epidemiology of medical error». BMJ. 320 (7237): 774–777. doi:10.1136/bmj.320.7237.774. PMC 1117772. PMID 10720365.
- ^ Friedman, Richard A.; D, M (2003). «CASES; Do Spelling and Penmanship Count? In Medicine, You Bet». The New York Times. Retrieved August 29, 2018.
- ^ Hannawa, Annegret F (June 2018). ««SACCIA Safe Communication»: Five core competencies for safe and high-quality care». Journal of Patient Safety and Risk Management. 23 (3): 99–107. doi:10.1177/2516043518774445. ISSN 2516-0435. S2CID 169364817.
- ^ Lyundup, Alexey V.; Balyasin, Maxim V.; Maksimova, Nadezhda V.; Kovina, Marina V.; Krasheninnikov, Mikhail E.; Dyuzheva, Tatiana G.; Yakovenko, Sergey A.; Appolonova, Svetlana A.; Schiöth, Helgi B.; Klabukov, Ilya D. (October 29, 2021). «Misdiagnosis of diabetic foot ulcer in patients with undiagnosed skin malignancies». International Wound Journal. 19 (4): 871–887. doi:10.1111/iwj.13688. ISSN 1742-481X. PMC 9013580. PMID 34713964. S2CID 240154096.
- ^ Aoki, Takuya; Watanuki, Satoshi (August 20, 2020). «Multimorbidity and patient-reported diagnostic errors in the primary care setting: multicentre cross-sectional study in Japan». BMJ Open. 10 (8): e039040. doi:10.1136/bmjopen-2020-039040. ISSN 2044-6055. PMC 7440713. PMID 32819954.
- ^ Maskell, Giles (2019). «Error in radiology—where are we now?». The British Journal of Radiology. 92 (1096): 20180845. doi:10.1259/bjr.20180845. PMC 6540865. PMID 30457880.
- ^ McGurk, S; Brauer, K; Macfarlane, TV; Duncan, KA (2008). «The effect of voice recognition software on comparative error rates in radiology reports». Br J Radiol. 81 (970): 767–70. doi:10.1259/bjr/20698753. PMID 18628322.
- ^ Wadhwa, R. R.; Park, D. Y.; Natowicz, M. R. (2018). «The accuracy of computer‐based diagnostic tools for the identification of concurrent genetic disorders». American Journal of Medical Genetics Part A. 176 (12): 2704–2709. doi:10.1002/ajmg.a.40651. PMID 30475443. S2CID 53758271.
- ^ Weingart SN (June 2000). «Epidemiology of medical error». Western Journal of Medicine. 172 (6): 390–3. doi:10.1136/ewjm.172.6.390. PMC 1070928. PMID 10854389.
- ^ «Feeding Tube Placement Devices Recalled After 23 Patient Deaths». schmidtlaw.com.
- ^ List of medical symptoms.
https://en.wikipedia.org/wiki/List_of_medical_symptoms#Medical_signs_and_symptoms - ^ Utter,GH; Atolagbe, OO; Cooke, DT. The Use of the International Classification of Diseases, Tenth Revision, Clinical Modification and Procedure Classification System in Clinical and Health Services Research; The Devil Is in the Details. JAMA Surgery. 2019;154(12):1089-1090
- ^ Emmett, KR. Nonspecific and atypical presentation of disease in the older patient. Geriatrics. 1998; 53(2):50–52
- ^ Ronicke, S; Hirsch, MC; Türk, E; Larionov, K; Tientcheu1, D; Wagne, AD. Can a decision support system accelerate rare disease diagnosis? Evaluating the potential impact of Ada DX in a retrospective study. Orphanet Journal of Rare Diseases. 2019. 14:69
- ^ a b c Neale, Graham; Woloshynowych, Maria; Vincent, Charles (July 2001). «Exploring the causes of adverse events in NHS hospital practice». Journal of the Royal Society of Medicine. 94 (7): 322–30. doi:10.1177/014107680109400702. PMC 1281594. PMID 11418700.
- ^ a b Gardner, Amanda (March 6, 2007). «Medication Errors During Surgeries Particularly Dangerous». The Washington Post. Retrieved March 13, 2007.
- ^ McDonald, MD, Clement J. (April 4, 2006). «Computerization Can Create Safety Hazards: A Bar-Coding Near Miss». Annals of Internal Medicine. 144 (7): 510–516. doi:10.7326/0003-4819-144-7-200604040-00010. PMID 16585665.
- ^ US Agency for Healthcare Research & Quality (January 9, 2008). «Physicians Want To Learn from Medical Mistakes but Say Current Error-reporting Systems Are Inadequate». Archived from the original on February 17, 2008. Retrieved March 23, 2008.
- ^ Clement JP; Lindrooth RC; Chukmaitov AS; Chen HF (February 2007). «Does the patient’s payer matter in hospital patient safety?: a study of urban hospitals». Med Care. 45 (2): 131–8. doi:10.1097/01.mlr.0000244636.54588.2b. PMID 17224775. S2CID 22206854.
- ^ «Incorporating Patient-Safe Design into the Guidelines». The American Institute of Architects Academy Journal. October 19, 2005.
- ^ The Joint Commission’s Annual Report on Quality and Safety 2007: Improving America’s Hospitals (Accessed 2008-04-09)
- ^ a b c d e Wu AW, Folkman S, McPhee SJ, Lo B (1991). «Do house officers learn from their mistakes?». JAMA. 265 (16): 2089–94. doi:10.1001/jama.265.16.2089. PMID 2013929.
- ^ Michael L. Millenson (2003). «The Silence». Health Affairs. 22 (2): 103–112. doi:10.1377/hlthaff.22.2.103. PMID 12674412. S2CID 40037135.
- ^ Henneman, Elizabeth A. (October 1, 2007). «Unreported Errors in the Intensive Care Unit, A Case Study of the Way We Work». Critical Care Nurse. 27 (5): 27–34. doi:10.4037/ccn2007.27.5.27. PMID 17901458. Retrieved March 23, 2008.
- ^ Phillips DP; Barker GE (May 2010). «A July Spike in Fatal Medication Errors: A Possible Effect of New Medical Residents». J Gen Intern Med. 25 (8): 774–779. doi:10.1007/s11606-010-1356-3. PMC 2896592. PMID 20512532.
- ^ Krupa, Carolyne (June 21, 2010). «New residents linked to July medication errors». American Medical News. 6 (21).
- ^ Jerome E. Groopman (November 5, 2009). «Diagnosis: What Doctors are Missing». New York Review of Books.
- ^ Croskerry, P. (2009). «A Universal Model of Clinical Reasoning». Acad Med. 84 (8): 1022–8. doi:10.1097/ACM.0b013e3181ace703. PMID 19638766.
- ^ a b Ker, Katharine; Edwards, Philip James; Felix, Lambert M; Blackhall, Karen; Roberts, Ian (May 12, 2010). «Caffeine for the prevention of injuries and errors in shift workers». Cochrane Database of Systematic Reviews. 2010 (5): CD008508. doi:10.1002/14651858.CD008508. PMC 4160007. PMID 20464765.
- ^ Barger, L. K.; et al. (2006). «Impact of Extended-Duration Shifts on Medical Errors, Adverse Events, and Attentional Failures». PLOS Med. 3 (12): e487. doi:10.1371/journal.pmed.0030487. PMC 1705824. PMID 17194188.
- ^ a b When Doctors Don’t Sleep, Talk of the Nation, National Public Radio, 13 December 2006.
- ^ Nocera, Antony; Khursandi, Diana Strange (June 1998). «Doctors’ working hours: can the medical profession afford to let the courts decide what is reasonable?». Medical Journal of Australia. 168 (12): 616–618. doi:10.5694/j.1326-5377.1998.tb141450.x. PMID 9673625. S2CID 34759813.
- ^ Landrigan, Christopher P.; Rothschild, Jeffrey M.; Cronin, John W.; Kaushal, Rainu; Burdick, Elisabeth; Katz, Joel T.; Lilly, Craig M.; Stone, Peter H.; Lockley, Steven W.; Bates, David W.; Czeisler, Charles A. (October 28, 2004). «Effect of Reducing Interns’ Work Hours on Serious Medical Errors in Intensive Care Units». New England Journal of Medicine. 351 (18): 1838–1848. doi:10.1056/NEJMoa041406. PMID 15509817.
- ^ Barger, Laura K; Ayas, Najib T; Cade, Brian E; Cronin, John W; Rosner, Bernard; Speizer, Frank E; Czeisler, Charles A; Mignot, Emmanuel (December 12, 2006). «Impact of Extended-Duration Shifts on Medical Errors, Adverse Events, and Attentional Failures». PLOS Medicine. 3 (12): e487. doi:10.1371/journal.pmed.0030487. PMC 1705824. PMID 17194188.
- ^ a b Pereira-Lima, K; Mata, DA; Loureiro, SR; Crippa, JA; Bolsoni, LM; Sen, S (2019). «Association Between Physician Depressive Symptoms and Medical Errors: A Systematic Review and Meta-analysis». JAMA Network Open. 2 (11): e1916097. doi:10.1001/jamanetworkopen.2019.16097. PMC 6902829. PMID 31774520.
- ^ Fahrenkopf, Amy M; Sectish, Theodore C; Barger, Laura K; Sharek, Paul J; Lewin, Daniel; Chiang, Vincent W; Edwards, Sarah; Wiedermann, Bernhard L; Landrigan, Christopher P (March 1, 2008). «Rates of medication errors among depressed and burnt out residents: prospective cohort study». BMJ. 336 (7642): 488–491. doi:10.1136/bmj.39469.763218.BE. PMC 2258399. PMID 18258931.
- ^ Aiken, Linda H.; Clarke, SP; Sloane, DM; Sochalski, J; Silber, JH (October 23, 2002). «Hospital Nurse Staffing and Patient Mortality, Nurse Burnout, and Job Dissatisfaction». JAMA. 288 (16): 1987–93. doi:10.1001/jama.288.16.1987. PMID 12387650.
- ^ 8th Annual MEDMARX Report (January 29, 2008). «Press Release». U.S. Pharmacopeia. Archived from the original on February 8, 2008. Retrieved March 23, 2008.
- ^ a b Waite, Stephen; Grigorian, Arkadij; Alexander, Robert G.; Macknik, Stephen L.; Carrasco, Marisa; Heeger, David J.; Martinez-Conde, Susana (June 25, 2019). «Analysis of Perceptual Expertise in Radiology – Current Knowledge and a New Perspective». Frontiers in Human Neuroscience. 13: 213. doi:10.3389/fnhum.2019.00213. PMC 6603246. PMID 31293407.
- ^ Alexander, Robert; Yazdanie, Fahd; Waite, Stephen Anthony; Chaudhry, Zeshan; Kolla, Srinivas; Macknik, Stephen; Martinez-Conde, Susana (2021). «Visual Illusions in Radiology: untrue perceptions in medical images and their implications for diagnostic accuracy». Frontiers in Neuroscience. 15: 629469. doi:10.3389/fnins.2021.629469. PMC 8226024. PMID 34177444.
- ^ Anderson, J.G. (2005). Information technology for detecting medication errors and adverse drug events. (Expert Opin Drug Saf 3). pp. 449–455.
- ^ Abrahamson, Kathleen; Anderson, J.G. (2017). «Your Health Care May Kill You: Medical Errors». Studies in Health Technology and Informatics. 234 (Building Capacity for Health Informatics in the Future): 13–17. doi:10.3233/978-1-61499-742-9-13. PMID 28186008.
{{cite journal}}: CS1 maint: url-status (link) - ^ Makary, Martin; Daniel, Michael (2016). «Medical error—the third leading cause of death in the US». BMJ. 353: i2139. doi:10.1136/bmj.i2139. PMID 27143499. S2CID 206910205.
- ^ Shreve, J et al (Milliman Inc.) (June 2010). «The Economic Measurement of Medical Errors» (PDF). Society of Actuaries.
- ^ Arlen, Jennifer (October 1, 2013). «Economic Analysis of Medical Malpractice Liability and Its Reform». New York University Law and Economics Working Papers. SSRN 2262792.
- ^ Berlin, Leonard (2007). «Accuracy of Diagnostic Procedures: Has It Improved Over the Past Five Decades?». American Journal of Roentgenology. 188 (5): 1173–1178. doi:10.2214/AJR.06.1270. PMID 17449754.
- ^ Brady, Adrian (December 7, 2016). «Error and discrepancy in radiology: inevitable or avoidable?». Insights into Imaging. 8 (1): 171–182. doi:10.1007/s13244-016-0534-1. PMC 5265198. PMID 27928712.
- ^ Brady, Adrian (January 2012). «Discrepancy and Error in Radiology: Concepts, Causes and Consequences». Ulster Med J. 81 (1): 3–9. PMC 3609674. PMID 23536732.
- ^ Siemieniuk, Reed; Fonseca, Kevin; Gill, M. John (November 2012). «Using Root Cause Analysis and Form Redesign to Reduce Incorrect Ordering of HIV Tests». Joint Commission Journal on Quality and Patient Safety. 38 (11): 506–512. doi:10.1016/S1553-7250(12)38067-7. PMID 23173397.
- ^ Berner, Eta S.; Graber, Mark L. (May 2008). «Overconfidence as a Cause of Diagnostic Error in Medicine». The American Journal of Medicine. 121 (5): S2–S23. doi:10.1016/j.amjmed.2008.01.001. PMID 18440350.
- ^ Weng, Qing Yu; Raff, Adam B.; Cohen, Jeffrey M.; Gunasekera, Nicole; Okhovat, Jean-Phillip; Vedak, Priyanka; Joyce, Cara; Kroshinsky, Daniela; Mostaghimi, Arash (February 1, 2017). «Costs and Consequences Associated With Misdiagnosed Lower Extremity Cellulitis». JAMA Dermatology. 153 (2): 141–146. doi:10.1001/jamadermatol.2016.3816. PMID 27806170. S2CID 205110504.
- ^ Bowden, Charles L. (January 2001). «Strategies to Reduce Misdiagnosis of Bipolar Depression». Psychiatric Services. 52 (1): 51–55. doi:10.1176/appi.ps.52.1.51. PMID 11141528.
- ^ «Schizophrenia Symptoms». schizophrenia.com. Retrieved March 30, 2008.
- ^ Dagan Y, Ayalon L (2005). «Case study: psychiatric misdiagnosis of non-24-hours sleep–wake schedule disorder resolved by melatonin». J Am Acad Child Adolesc Psychiatry. 44 (12): 1271–1275. doi:10.1097/01.chi.0000181040.83465.48. PMID 16292119.
- ^ van Vliet, J A; Eekers, PJ; Haan, J; Ferrari, MD; Dutch RUSSH Study, Group. (August 1, 2003). «Features involved in the diagnostic delay of cluster headache». Journal of Neurology, Neurosurgery & Psychiatry. 74 (8): 1123–1125. doi:10.1136/jnnp.74.8.1123. PMC 1738593. PMID 12876249.
- ^ «IHS Classification ICHD-II 3.1 Cluster headache». The International Headache Society. Archived from the original on 3 November 2013. Retrieved 3 January 2014.
- ^ Tfelt-Hansen, Peer C.; Jensen, Rigmor H. (July 2012). «Management of Cluster Headache». CNS Drugs. 26 (7): 571–580. doi:10.2165/11632850-000000000-00000. PMID 22650381. S2CID 22522914.
- ^ Brett, Denise; Warnell, Frances; McConachie, Helen; Parr, Jeremy R. (2016). «Factors Affecting Age at ASD Diagnosis in UK: No Evidence that Diagnosis Age has Decreased Between 2004 and 2014». Journal of Autism and Developmental Disorders. 46 (6): 1974–1984. doi:10.1007/s10803-016-2716-6. PMC 4860193. PMID 27032954.
- ^ Lehnhardt, F.-G.; Gawronski, A.; Volpert, K.; Schilbach, L.; Tepest, R.; Vogeley, K. (November 15, 2011). «Das psychosoziale Funktionsniveau spätdiagnostizierter Patienten mit Autismus-Spektrum-Störungen – eine retrospektive Untersuchung im Erwachsenenalter» [Psychosocial functioning of adults with late diagnosed autism spectrum disorders—a retrospective study]. Fortschritte der Neurologie · Psychiatrie (in German). 80 (2): 88–97. doi:10.1055/s-0031-1281642. PMID 22086712.
- ^ Aggarwal, Shilpa; Angus, Beth (February 4, 2015). «Misdiagnosis versus missed diagnosis: diagnosing autism spectrum disorder in adolescents». Australasian Psychiatry. 23 (2): 120–123. doi:10.1177/1039856214568214. PMID 25653302. S2CID 43475267.
- ^ Corvin, Aiden; Fitzgerald, Michael (2001). «Diagnosis and differential diagnosis of Asperger syndrome». Advances in Psychiatric Treatment. 7 (4): 310–318. doi:10.1192/apt.7.4.310.
- ^ Leskovec, Thomas J.; Rowles, Brieana M.; Findling, Robert L. (March 2008). «Pharmacological Treatment Options for Autism Spectrum Disorders in Children and Adolescents». Harvard Review of Psychiatry. 16 (2): 97–112. doi:10.1080/10673220802075852. PMID 18415882. S2CID 26112061.
- ^ «Reliability and Prevalence in the DSM-5 Field Trials» (PDF). January 12, 2012. Archived from the original (PDF) on January 31, 2012. Retrieved January 13, 2012.
- ^ Linda T. Kohn; Janet M. Corrigan; Molla S. Donaldson (2000). To Err is Human: Building a Safer Health System. doi:10.17226/9728. ISBN 978-0-309-26174-6. PMID 25077248.
- ^ a b Raden Anita Indriyanti; Fajar Awalia Yulianto; Yuke Andriane (2019). «Prescription Writing Errors in Clinical Clerkship among Medical Students» (PDF). Global Medical and Health Communication. 7: 41–42. doi:10.29313/gmhc.v7i1.4069. ISSN 2301-9123. OCLC 8186593909. Archived from the original on September 26, 2020 – via DOAJ.
- ^ «APPEAL NO. 991681 Texas v. Dr. K» (PDF). Retrieved April 16, 2020.
- ^ Elliott, Rachel (February 22, 2018). «PREVALENCE AND ECONOMIC BURDEN OF MEDICATION ERRORS IN THE NHS IN ENGLAND» (PDF). University of Sheffield. Policy Research Unit in Economic Evaluation of Health & Care Interventions. Retrieved June 19, 2022.
- ^ https://academic.oup.com/ijpp/article/28/6/663/6133310?login=false.
- ^ Coutsouvelis, John; Siderov, Jim; Tey, Amanda Y.; Bortz, Hadley D.; o’Connor, Shaun R.; Rowan, Gail D.; Vasileff, Hayley M.; Page, Amy T.; Percival, Mia A. (2020). «The impact of pharmacist‐led strategies implemented to reduce errors related to cancer therapies: A systematic review». Journal of Pharmacy Practice and Research. 50 (6): 466–480. doi:10.1002/jppr.1699. S2CID 229332634.
- ^ Donyai, Parastou (February 2008). «The effects of electronic prescribing on the quality of prescribing». British Journal of Clinical Pharmacology. Br J Clin Pharmacol. 65 (2): 230–237. doi:10.1111/j.1365-2125.2007.02995.x. PMC 2253693. PMID 17662088.
- ^ Hilfiker D (1984). «Facing our mistakes». N. Engl. J. Med. 310 (2): 118–22. doi:10.1056/NEJM198401123100211. PMID 6690918.
- ^ Christensen JF, Levinson W, Dunn PM (1992). «The heart of darkness: the impact of perceived mistakes on physicians». Journal of General Internal Medicine. 7 (4): 424–31. doi:10.1007/bf02599161. PMID 1506949. S2CID 415258.
- ^ Wu AW (2000). «Medical error: the second victim : The doctor who makes the mistake needs help too». BMJ. 320 (7237): 726–7. doi:10.1136/bmj.320.7237.726. PMC 1117748. PMID 10720336.
- ^ Waterman AD, Garbutt J, Hazel E, Dunagan WC, Levinson W, Fraser VJ, Gallagher TH (2007). «The Emotional Impact of Medical Errors on Practicing Physicians in the United States and Canada». Joint Commission Journal on Quality and Patient Safety. 33 (2): 467–476. doi:10.1016/S1553-7250(07)33050-X. PMID 17724943.
- ^ a b Dean B, Barber N, Schachter M (October 2000). «What is a prescribing error?». Qual Saf Health Care. 9 (4): 232‐237. doi:10.1136/qhc.9.4.232. PMC 1743540. PMID 11101708.
- ^ a b c Romero‐Perez, Raquel; Hildick‐Smith, Philippa (September 2012). «Minimising Prescribing Errors in Paediatrics ‐ Clinical Audit» (PDF). Scottish Universities Medical Journal. 1: 14–1.
- ^ Gandhi, Tejal K.; Kachalia, Allen; Thomas, Eric J.; Puopolo, Ann Louise; Yoon, Catherine; Brennan, Troyen A.; Studdert, David M. (October 3, 2006). «Missed and Delayed Diagnoses in the Ambulatory Setting: A Study of Closed Malpractice Claims». Annals of Internal Medicine. 145 (7): 488–96. doi:10.7326/0003-4819-145-7-200610030-00006. PMID 17015866. S2CID 29006252.
- ^ Redelmeier, Donald A.; Tan, Siew H.; Booth, Gillian L. (May 21, 1998). «The Treatment of Unrelated Disorders in Patients with Chronic Medical Diseases». New England Journal of Medicine. 338 (21): 1516–1520. doi:10.1056/NEJM199805213382106. PMID 9593791.
- ^ Lurie, Nicole; Rank, Brian; Parenti, Connie; Woolley, Tony; Snoke, William (June 22, 1989). «How Do House Officers Spend Their Nights?». New England Journal of Medicine. 320 (25): 1673–1677. doi:10.1056/NEJM198906223202507. PMID 2725617.
- ^ Lyle CB, Applegate WB, Citron DS, Williams OD (1976). «Practice habits in a group of eight internists». Ann. Intern. Med. 84 (5): 594–601. doi:10.7326/0003-4819-84-5-594. PMID 1275366.
- ^ Thomas Laurence (2004). «What Do You Want?». Extreme Clinic — An Outpatient Doctor’s Guide to the Perfect 7 Minute Visit. Philadelphia: Hanley & Belfus. p. 120. ISBN 978-1-56053-603-1.
- ^ a b Seder D (2006). «Of poems and patients». Ann. Intern. Med. 144 (2): 142. doi:10.7326/0003-4819-144-2-200601170-00014. PMID 16418416. S2CID 2927435.
- ^ Berlinger, N; Wu, AW (February 1, 2005). «Subtracting insult from injury: addressing cultural expectations in the disclosure of medical error». Journal of Medical Ethics. 31 (2): 106–108. doi:10.1136/jme.2003.005538. PMC 1734098. PMID 15681676.
- ^ a b «Medical Error Disclosure Competence (MEDC) — Prof. Dr. Annegret Hannawa». prof. annegret hannawa. Retrieved April 21, 2021.
- ^ West, Colin P.; Huschka, Mashele M.; Novotny, Paul J.; Sloan, Jeff A.; Kolars, Joseph C.; Habermann, Thomas M.; Shanafelt, Tait D. (September 6, 2006). «Association of Perceived Medical Errors With Resident Distress and Empathy». JAMA. 296 (9): 1071–8. doi:10.1001/jama.296.9.1071. PMID 16954486.
- ^ Wu AW, Folkman S, McPhee SJ, Lo B (1993). «How house officers cope with their mistakes». West. J. Med. 159 (5): 565–9. PMC 1022346. PMID 8279153.
- ^ Gallagher TH, Waterman AD, Ebers AG, Fraser VJ, Levinson W (2003). «Patients’ and physicians’ attitudes regarding the disclosure of medical errors». JAMA. 289 (8): 1001–7. doi:10.1001/jama.289.8.1001. PMID 12597752.
- ^ Rosemary Gibson; Janardan Prasad Singh (2003). Wall of Silence. Regnery. ISBN 978-0-89526-112-0.
- ^ Wu, Albert W.; Cavanaugh, Thomas A.; McPhee, Stephen J.; Lo, Bernard; Micco, Guy P. (December 1997). «To tell the truth». Journal of General Internal Medicine. 12 (12): 770–775. doi:10.1046/j.1525-1497.1997.07163.x. PMC 1497204. PMID 9436897.
- ^ Kelly, Karen (2005). «Study explores how physicians communicate mistakes». University of Toronto. Archived from the original on March 22, 2006. Retrieved March 17, 2006.
- ^ Agency for Healthcare Research and Quality (AHRQ) http://psnet.ahrq.gov/primer.aspx?primerID=2
- ^ Snyder L, Leffler C (2005). «Ethics manual: fifth edition». Ann Intern Med. 142 (7): 560–82. doi:10.7326/0003-4819-142-7-200504050-00014. PMID 15809467. S2CID 53090205.
- ^ Kaldjian LC, Jones EW, Wu BJ, Forman-Hoffman VL, Levi BH, Rosenthal GE (2007). «Disclosing Medical Errors to Patients: Attitudes and Practices of Physicians and Trainees». Journal of General Internal Medicine. 22 (7): 988–96. doi:10.1007/s11606-007-0227-z. PMC 2219725. PMID 17473944.
- ^ Weissman JS, Annas CL, Epstein AM, et al. (2005). «Error reporting and disclosure systems: views from hospital leaders». JAMA. 293 (11): 1359–66. doi:10.1001/jama.293.11.1359. PMID 15769969.
- ^ Wu AW (1999). «Handling hospital errors: is disclosure the best defense?». Ann. Intern. Med. 131 (12): 970–2. doi:10.7326/0003-4819-131-12-199912210-00012. PMID 10610651. S2CID 36889006.
- ^ Zimmerman R (May 18, 2004). «Doctors’ New Tool To Fight Lawsuits: Saying ‘I’m Sorry’«. The Wall Street Journal. p. A1. Archived from the original on August 23, 2007.
- ^ Newman MC (1996). «The emotional impact of mistakes on family physicians». Archives of Family Medicine. 5 (2): 71–5. doi:10.1001/archfami.5.2.71. PMID 8601210.
- ^ a b Sobecks, Nancy W.; Justice, AC; Hinze, S; Chirayath, HT; Lasek, RJ; Chren, MM; Aucott, J; Juknialis, B; Fortinsky, R; Youngner, S; Landefeld, CS (February 16, 1999). «When Doctors Marry Doctors: A Survey Exploring the Professional and Family Lives of Young Physicians». Annals of Internal Medicine. 130 (4_Part_1): 312–9. doi:10.7326/0003-4819-130-4-199902160-00017. PMID 10068390.
- ^ Oscar London (1987). «Rule 35: Don’t Take Too Much Joy in the Mistakes of Other Doctors». Kill as few patients as possible: and fifty-six other essays on how to be the world’s best doctor. Berkeley, Calif: Ten Speed Press. ISBN 978-0-89815-197-8.
- ^ Barach, P.; Small, SD (March 18, 2000). «Reporting and preventing medical mishaps: lessons from non-medical near miss reporting systems». BMJ. 320 (7237): 759–763. doi:10.1136/bmj.320.7237.759. PMC 1117768. PMID 10720361.
- ^ Banja, John D. (2005). Medical errors and medical narcissism. Sudbury, Massachusetts: Jones and Bartlett. ISBN 978-0-7637-8361-7.
- ^ Weiss, Gail Garfinkel (January 4, 2011). «‘Some Worms Are Best Left in the Can’ — Should You Hide Medical Errors?». Medscape.
- ^ Helmreich, R. L (March 18, 2000). «On error management: lessons from aviation». BMJ. 320 (7237): 781–785. doi:10.1136/bmj.320.7237.781. PMC 1117774. PMID 10720367.
- ^ Espinosa, J. A; Nolan, TW (March 18, 2000). «Reducing errors made by emergency physicians in interpreting radiographs: longitudinal study». BMJ. 320 (7237): 737–740. doi:10.1136/bmj.320.7237.737. PMC 27314. PMID 10720354.
- ^ Relihan, Eileen C; Silke, Bernard; Ryder, Sheila A (June 23, 2012). «Design template for a medication safety programme in an acute teaching hospital». European Journal of Hospital Pharmacy. 19 (3): 340–344. doi:10.1136/ejhpharm-2012-000050. hdl:2262/66780. S2CID 54178056.
- ^ Alam, Rabiul (2016). «Spinal needle with prefilled syringe to prevent medication error: A proposal». Indian Journal of Anaesthesia. 60 (7): 525–7. doi:10.4103/0019-5049.186014. PMC 4966365. PMID 27512177.
- ^ West, Colin P (2016). «Physician Well-Being: Expanding the Triple Aim». Journal of General Internal Medicine. 31 (5): 458–459. doi:10.1007/s11606-016-3641-2. PMC 4835383. PMID 26921157.
- ^ Hanlon, Carrie; Sheedy, Kaitlin; Kniffin, Taylor; Rosenthal, Jill (2015). «2014 Guide to State Adverse Event Reporting Systems» (PDF). NASHP.org. National Academy for State Health Policy. Retrieved April 22, 2016.
- ^ «A national survey of medical error reporting laws» (PDF). Yale Journal of Health Policy, Law, and Ethics. 9 (1): 201–86. 2009. PMID 19388488. Retrieved April 22, 2016.
- ^ «Report Finds Most Errors at Hospitals Go Unreported» article by Robert Pear in The New York Times January 6, 2012
- ^ Summary «Hospital Incident Reporting Systems Do Not Capture Most Patient Harm» Report (OEI-06-09-00091) Office of Inspector General, Department of Health and Human Services, January 6, 2012
- ^ Gaba, David M. (March 18, 2000). «Anaesthesiology as a model for patient safety in health care». BMJ. 320 (7237): 785–788. doi:10.1136/bmj.320.7237.785. PMC 1117775. PMID 10720368.
- ^ Barnsteiner, Jane H. (2008), Hughes, Ronda G. (ed.), «Medication Reconciliation», Patient Safety and Quality: An Evidence-Based Handbook for Nurses, Advances in Patient Safety, Rockville (MD): Agency for Healthcare Research and Quality (US), PMID 21328749, retrieved July 17, 2023
- ^
- ^ Pease E (1936). «Minimum standards for a hospital pharmacy». Bull Am Coll Surg. 21: 34–35.
- ^ Garrison TJ (1979). Smith MC; Brown TR (eds.). IV.1 Medication Distribution Systems. ISBN 978-0-683-07884-8.
- ^ Woodward WA; Schwartau N (1979). Smith MC; Brown TR (eds.). Chapter IV.3 Developing Intravenous Admixture Systems. ISBN 978-0-683-07884-8.
- ^ Powell MF (1986). Smith MC; Brown TR (eds.). Chapter 53 The Patient Profile System. ISBN 978-0-683-01090-9.
- ^ Evens RP (1986). Smith MC; Brown TR (eds.). Chapter 31 Communicating Drug Information. ISBN 978-0-683-01090-9.
- ^ Gorski DH (February 4, 2019). «Are medical errors really the third most common cause of death in the U.S.? (2019 edition)». Science-Based Medicine.
- ^ René Amalberti; Yves Auroy; Don Berwick; Paul Barach (May 3, 2005). «Five System Barriers to Achieving Ultrasafe Health Care». Annals of Internal Medicine. 142 (9): 756–764. doi:10.7326/0003-4819-142-9-200505030-00012. PMID 15867408.
Further reading[edit]
- Gawande, Atul (2002). Complications: A Surgeon’s Notes on an Imperfect Science. New York: Metropolitan Books. ISBN 978-0-8050-6319-6.
- Wachter, Robert; Shojania, Kaveh (2004). Internal Bleeding: The Truth Behind America’s Terrifying Epidemic of Medical Mistakes. New York: Rugged Land. ISBN 978-1-59071-016-6.
- Banja, John (2005). Medical Errors and Medical Narcissism. Boston: Jones and Bartlett. ISBN 978-0-7637-8361-7.
- Porter, Michael E.; Olmsted Teisberg, Elizabeth (2006). Redefining Health Care: Creating Value-Based Competition on Results. Boston: Harvard Business School Press. ISBN 978-1-59139-778-6.
- Gibson, Rosemary; Prasad Singh, Janardan (2003). Wall of Silence: The Untold Story of the Medical Mistakes That Kill and Injure Millions of Americans. Washington D.C.: Regnery. ISBN 978-0-89526-112-0.
- Alldred D.P.; Standage C.; Zermansky A.G.; Jesson B.; Savage I.; Franklin B.D.; Barber N.; Raynor D.K. (2008). «Development and validation of criteria to identify medication-monitoring errors in care home residents». International Journal of Pharmacy Practice. 16 (5): 317–323. doi:10.1211/ijpp.16.5.0007. S2CID 71701489.
- Committee on Identifying and Preventing Medication Errors; Board on Health Care Services (2007). Preventing medication errors. National Academies Press. ISBN 978-0-309-10147-9.
- Tewari, A.; Palm, B.; Hines, T.; Royer, T.; Alexander, E. (2014). «VEINROM: A possible solution for erroneous intravenous drug administration». Journal of Anaesthesiology Clinical Pharmacology. 30 (2): 263–266. doi:10.4103/0970-9185.130055. PMC 4009652. PMID 24803770.
Врачи – те люди, которые посвятили свою жизнь охране здоровья сограждан. Именно они самоотверженно бросаются в жерло эпидемий, разрабатывают новые лекарства, проводят многочасовые операции. Врачебная деятельность изматывает и истощает. Уставший человек, как известно, склонен совершать ошибки. Иногда, к сожалению, происходит так, что ошибка врача стоит его пациенту жизни.
Понятие врачебной ошибки
Самого по себе понятия «врачебная ошибка» в российском законодательстве нет. Однако существует её бытовое понимание. Врачебной ошибкой называется ошибка медицинского специалиста в выполнении его обязанностей. Врачебную ошибку обуславливают халатность или небрежность действий. Помимо этого, в понятие «врачебной ошибки» входят ненадлежаще выполненные действия или бездействие медицинского работника. Суммируя, можно сказать, что медицинская ошибка – это неверные действия врача или иного медицинского персонала, которые повлекли за собой ухудшение здоровья пациента или его смерть.
Какие бывают врачебные ошибки
В целом, можно выделить шесть видов медицинских ошибок:
- 1.Диагностическая ошибка. Пациенту изначально был поставлен неверный диагноз.
- 2.Лечебно-техническая ошибка. Метод исследования, позволяющий поставить диагноз, был выбран неверно.
- 3.Лечебно-тактическая ошибка. Результаты исследования были неверно интерпретированы.
- 4.Организационная ошибка. В случае этой ошибки неверно был организован лечебный процесс, не хватало медицинского персонала.
- 5.Документационная ошибка. Под этой ошибкой понимается ситуация, когда предпринятые в отношении пациента действия не были письменно зафиксированы, документация велась неверно.
- 6.Ненадлежащее поведение медицинских служащих. Во время совершения этой ошибки, медицинский персонал пренебрег нормами этики и морали в отношении пациентов.
В России не ведётся официальная статистика медицинских ошибок, поэтому предположить, сколько людей в год погибает из-за халатности медицинского персонала не представляется возможным.
Ответственность за врачебные ошибки
Врач, совершивший ошибку, будет отстранен администрацией больницы от работы, уволен или вовсе окажется в местах лишения свободы. Медицинское учреждение, в котором работал провинившийся врач, должно будет возместить ущерб родственникам почившего в материальном эквиваленте. В случае нанесения вреда здоровью пациента это может быть бесплатное лечение, санаторий, приобретение инвалидной коляски или протеза и т.д. Если же в результате врачебной ошибки пациент умирает, то его семья получает денежную компенсацию в объёме, устанавливаемом судом.
Куда идти, если есть подозрение на врачебную ошибку?
Если вам кажется, что вашего близкого неправильно лечат, то вам следует посетить отделение главврача, где будет произведено назначение нового лечащего врача. Если этого не происходит, есть смысл обратиться в другое медицинское учреждение, где будет выдана справка о том, что лечение осуществлялось некорректно. Далее следует идти в Минздрав субъекта РФ или в Роспотребнадзор и заявлять о необходимости проверки в медицинском учреждении, не оказавшем должные медицинские услуги.
В результате врачебной ошибки может наступить и смерть. Если есть подозрение на ошибку, то вы не сможете отказаться от вскрытия почившего. Необходимо чтобы патологоанатом осмотрел его и вынес вердикт о наличии или отсутствии врачебной ошибки.
Когда уже поздно обращаться в суд?
Если вы хотите отстаивать свои права в суде, то нужно обратиться в него не позднее 3 лет с момента того как вы узнали о нарушении прав. В случае медицинских ошибок срок исковой давности начинает исчисляться начиная с дат неверных медицинских диагнозов, дат заключений других специалистов и т.д.
6 октября 2021
Возможно, вам будет интересно:
- Статистика смертности в России
- Как избежать смерти от сердечно-сосудистых заболеваний
- Борьба с болью утраты